Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Az ISZB kialakulása. Preklinikus szakasz
Response-to-injury elmélet A preklinikus fázis évtizedekig tart. (20-30 éves USA vadászpilóták boncolásakor 10%-ban találtak ISZB-t a koreai háború alatt ) Rizikó faktorok (lipidek, dohányzás, hypertonia, diabetes, obesitas, stress, inaktív életmód, férfi nem) Infekciók?
 Rizikó faktorok (lipidek, dohányzás, hypertonia, diabetes, obesitas, stress, inaktív életmód, férfi nem) Infekciók")
2
CARDIOVASCULARIS PRIORITÁSOK SZINTJEI
Kifejlődött koszorúér-betegség, perifériás érbetegség és cerebrovascularis érbetegség Nagy kockázatú, tünetmentes egyének A rizikófaktorok együttesen 10 évre >5%-os fatális CV eseményt valószínűsítenek Az egyes rizikófaktorok szintje igen magas: össz koleszterin: >8 mmol/l, LDL-koleszterin: >6 mmol/l, RR>180/110 Hgmm 2-es típusú DM, vagy 1-es típusú DM mikroalbuminuriával Közeli vérrokonánál Korai atheroscleroticus betegség előfordult Tünetmentes, de nagy kockázat állapítható meg Mindenki más, aki az orvosánál megjelenik

3
SCORE RENDSZER Nem Életkor Dohányzás Systolés RR Koleszterin
Alacsony vagy magas rizikójú ország Eur Heart J.2003;24:

4
1. MAGATARTÁSI RIZIKÓFAKTOROK LEKÜZDÉSÉNEK STRATÉGIÁJA
Alakítsunk ki a beteggel terápiás szövetséget A beteg értse meg az életmód és az egészség kapcsolatát Ismerje meg a változtatás gátjait Akarja a változásokat Az orvossal együtt döntse el a változtatások sorrendjét Ellenőrizzük az eredményeket Vegyünk igénybe professzionális segítséget

5
2. A DOHÁNYZÁS ABBAHAGYÁSA
Minden orvos-beteg kapcsolatkor rá kell kérdezni a dohányzásra Meg kell határozni a betegek dohányzáshoz való hozzászokásának a mértékét és a leszokási készségüket Erősen ösztökélni kell minden dohányost a leszokásra Meg kell a beteggel beszélni a leszokás stratégiáját, amibe a magatartási tanácsok adásán kívül beletartozik a nikotinpótló és/vagy gyógyszeres kezelés is Rendszeresen ellenőrizni kell a beteget

6
3. EGÉSZSÉGES TÁPLÁLKOZÁS
A kalóriabevitelt az ideális testsúly fenntartásához kell adaptálni Ajánlott táplálékok: gyümölcs, zöldség, teljes őrlésű gabona és kenyér, alacsony zsírtartalmú diétás anyagok, hal és sovány hús A halolaj és az omega-3 zsírsavaknak protektív hatásuk van A kalóriabevitel 30%-át ne haladja meg a zsírfogyasztás, és annak egyharmadánál ne legyen nagyobb a telített zsírok bevitele. A napi koleszterin bevitel ne legyen több 300 mg-nál. A telített zsírokat részben komplex szénhidrátok, egyszeres vagy többszörösen telítetlen zsírok (zöldségek, tengeri halak) váltsák fel testsúly-, vérnyomáscsökkentés, a vércukorra, vérlipidszintekre való kedvező hatás és a trombózishajlam csökkenése
 váltsák fel. testsúly-, vérnyomáscsökkentés, a vércukorra, vérlipidszintekre való kedvező hatás és a trombózishajlam csökkenése.")
7
4. A FIZIKAI AKTIVITÁS NÖVELÉSE
Cél a hét minél több napján legalább fél óra fizikai aktivitás Egészséges emberek heti 4-5 alkalommal percig végezzenek olyan aktivitást, amelynek során az átlagos maximális szívfrekvencia 60-75%-át elérik. Betegeken előzetes terheléses teszt alapján kell a terhelés mértékét meghatározni.

8
5. TÚLSÚLY ÉS OBESITAS A testsúly csökkentése szükséges
Obesitas (BMI>30 kg/m2) Túlsúly (BMI>25 kg/m2) Derékkörfogat: férfiaknál>102 cm, nőknél>88 cm)
 Túlsúly (BMI>25 kg/m2) Derékkörfogat: férfiaknál>102 cm, nőknél>88 cm)")
9
AZ INTER-HEART STUDY RIZIKÓ FAKTORAI
személy, 62 vizsgáló hely, 52 ország 9 befolyásolható rizikó faktor felelős az infarktusok 90%-áért

10
AZ INTER-HEART STUDY RIZIKÓ FAKTORAI
ApoB/ApoA1 arány Dohányzás (jelenleg is) Diabétesz Hypertonia Abdominális elhízás Psychoszociális status Zöldség és gyümölcs fogyasztás hiánya Testmozgás hiánya Túlzott alkohol fogyasztás Ezen rizikó faktorok jelentősége földrajzi hovatartozástól és nemtől függetlenül, minden etnikai csoportban azonos mértékű.
 Diabétesz. Hypertonia. Abdominális elhízás. Psychoszociális status. Zöldség és gyümölcs fogyasztás hiánya. Testmozgás hiánya. Túlzott alkohol fogyasztás. Ezen rizikó faktorok jelentősége földrajzi hovatartozástól és. nemtől függetlenül, minden etnikai csoportban azonos mértékű.")
13
Kezelés. ISZB prevenció
A nyugati világban az ISZB halálozása %-kal csökkent az elmúlt évben A csökkenés fő oka a prevenció: dohányzás elhagyása, zsír és cholesterinszegény, kalóriaszegény diéta, rendszeres testmozgás a hypertonia és a diabetes körültekintő kezelése

14
ISZB. Klinikai szakasz, klinikai megjelenési formák
Nincs plakk ruptúra Stabil effort angina pectoris. Arrhythmiák. Szívelégtelenség Plakk ruptúra, acut coronaria syndromák instabil angina nonST elevációs myocardialis infarctus ST elevációs myocardialis infarctus

15
Mit tegyen a családorvos angina pectorisra utaló panaszok esetén?
Vegyen fel részletes anamnézist és rögzítse a fizikális statust Amennyiben a panasz típusos és új keletű (<30 nap), akkor az állapot instabilnak tekinthető és hospitalizáció szükséges Amennyiben hosszabb ideje fennálló panaszokról van szó, ill. a panaszok atipusosak Készítsen EKG-t Javasoljon rövid hatású Ngl.-t, amit a beteg panasz esetén használ Végeztesse el az alapvető labor vizsgálatokat Állapítsa meg, hogy a betegnek milyen rizikó faktorai vannak és kezdje meg azok befolyásolását/kezelését A korrekt diagnózis és a prognózis megállapítása érdekében küldje a beteget kardiológushoz
, akkor az állapot instabilnak tekinthető és hospitalizáció szükséges. Amennyiben hosszabb ideje fennálló panaszokról van. szó, ill. a panaszok atipusosak. Készítsen EKG-t. Javasoljon rövid hatású Ngl.-t, amit a beteg panasz esetén használ. Végeztesse el az alapvető labor vizsgálatokat. Állapítsa meg, hogy a betegnek milyen rizikó faktorai vannak és kezdje meg azok befolyásolását/kezelését. A korrekt diagnózis és a prognózis megállapítása érdekében küldje a beteget kardiológushoz.")
16
ISZB (plakk ruptúra nélkül), kezelés
Revaszkularizáció, többág-betegség esetén Gyógyszeres (revasc-val, vagy anélkül) stratégiai szerek (ASA, béta blockolók, /statinok, ACE-gátlók/) tüneti szerek (nitrátok, Ca-antagonisták, trimetazidin)
 stratégiai szerek (ASA, béta blockolók, /statinok, ACE-gátlók/) tüneti szerek (nitrátok, Ca-antagonisták, trimetazidin)")
17
Angina pectorisos beteg gondozása
1. ASA, NG, lipidcsökkentő 2. Tolerálja-e a béta blockolót? Ha igen, első antianginás szer a béta blockoló. 3. Ha nem tolerálja, vagy további antianginás kezelést indokolnak a panaszok: hosszú hatású nitrátkészitmény, és/vagy hosszú hatású Ca antagonista adása

19
Effects of alternative antihypertensive classes on regression of LV mass
–5 –10 –15 Change in LV mass index (%) More recent meta-analyses have suggested that regression of left ventricular mass with calcium channel blockers and ACE inhibitors are equivalent, and that both are superior to that achieved with diuretics and β-blockers (Schlaich M and Schmieder R. Am J Hypertens 1998). This observation is entirely compatible with the results from the PRESERVE study (Devereux R et al. Circulation 2001). Devereux RB, Palmieri V, Sharpe N, et al. Effects of once-daily angiotensin-converting enzyme inhibition and calcium channel blockade-based antihypertensive treatment regimens on left ventricular hypertrophy and diastolic filling in hypertension. The prospective randomized enalapril study evaluating regression of ventricular enlargement (PRESERVE) trial. Circulation 2001;104:1248–54. Schlaich MP, Schmieder RE. Left ventricular hypertrophy and its regression: pathophysiology and therapeutic approach: focus on treatment by antihypertensive agents. Am J Hypertens 1998;11:1394–404. p<0.05 p<0.05 Diuretics β-blockers CCBs ACE-Is Modified from Schlaich M, Schmieder R. Am J Hypertens 1998;11:1394–404.
 More recent meta-analyses have suggested that regression of left ventricular mass with calcium channel blockers and ACE inhibitors are equivalent, and that both are superior to that achieved with diuretics and β-blockers (Schlaich M and Schmieder R. Am J Hypertens 1998). This observation is entirely compatible with the results from the PRESERVE study (Devereux R et al. Circulation 2001). Devereux RB, Palmieri V, Sharpe N, et al. Effects of once-daily angiotensin-converting enzyme inhibition and calcium channel blockade-based antihypertensive treatment regimens on left ventricular hypertrophy and diastolic filling in hypertension. The prospective randomized enalapril study evaluating regression of ventricular enlargement (PRESERVE) trial. Circulation 2001;104:1248–54. Schlaich MP, Schmieder RE. Left ventricular hypertrophy and its regression: pathophysiology and therapeutic approach: focus on treatment by antihypertensive agents. Am J Hypertens 1998;11:1394–404. p<0.05. p<0.05. Diuretics. β-blockers. CCBs. ACE-Is. Modified from Schlaich M, Schmieder R. Am J Hypertens 1998;11:1394–404.")
20
Angiotensin II Norepinephrine Hypertrophy, apoptosis, ischaemia, arrhythmias, remodelling, fibrosis

21
Treatments to reduce mortality in heart failure
ACE inhibitors 39 trials n=8308 1361 deaths OR: 24% NNT/year: 74 b blockers 28 trials n=13 804 1432 deaths OR: 36% NNT/year: 29 ACE inhibitors and b blockers NNT/year: 21 Cleland & Freemantle (1999)
")
22
% mortality D ejection fraction D +30 PDE inhibitors +15 Digitalis
. . Amlodipine -15 ACE inhibition -30 b blockade -45 +0.01 +0.02 +0.03 +0.04 +0.05 +0.06 +0.07 ejection fraction D

23
HOPE - Kaplan-Meier Estimates of the Composite Endpoint of CV Death, MI or Stroke in the Ramipril and Placebo Groups P<0.001 N Engl J Med, January 20, 2000

24
Calcium Channel Blockers Multicenter Diltiazem Post-Infarction Trial (MDPIT)* EF <40%
*Subgroup analysis of patients with EF < 40% The Multicenter Diltiazem Post Infarction Trial Study Group N Engl J Med., 1988;319:385-92

25
A nifedipin GITS javítja a fő CV eredményeket
Végpont 0.41 0.62 0.18 0.015 0.10 0.073 Kockázat aránya (95% CI) p 1.07 (0.91–1.25) 1.04 (0.88–1.24) 0.86 (0.69–1.07) 0.71 (0.54–0.94) 0.78 (0.58–1.05) 1.25 (0.98–1.59) 0.5 1 1.5 2 Halál MI Refrakter angina Szívelégtelenség Stroke Perifériás revaszkularizáció nifedipin GITS-nek kedvez placebonak kedvez Említésre méltó, hogy a nifedipin GITS 29%-kal csökkentette (p=0.015) az új manifeszt szívelégtelenség előfordulását. Ez egy nemvárt eredmény volt, melyet az isémiás epizódok hosszútávú csökkenése és ezen kívül a folyamatos csökkentett vérnyomás magyarázhat. A nifedipin GITS csoportban a stroke előfordulása 22%-kal csökkent (p=0.10). A növekvő vérnyomás és a stroke előfordulása között fennálló kapcsolat régóta bizonyított.1 Annak az oka, hogy ez az ACTION-ben nem érte el a statisztikai szignifikancia szintjét a járulékos vérnyomáscsökkenés nem elegendő mértéke, illetve a stroke szigorú definíciója volt. A nifedipin GITS kezeléssel együtt járt a refrakter angina előfordulásának csökkenő tendenciája a placebohoz hasonlítva (150 ill. 174, p=0.18). Ez fontos megfigyelés, mert a refrakter angina a betegség előrehaladásának jele, és instablisis angina vagy MI kialakulásának megnövekedett kockázata kapcsolódik hozzá. 1. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903–13.
 p (0.91–1.25) 1.04 (0.88–1.24) 0.86 (0.69–1.07) 0.71 (0.54–0.94) 0.78 (0.58–1.05) 1.25 (0.98–1.59) Halál. MI. Refrakter angina. Szívelégtelenség. Stroke. Perifériás revaszkularizáció. nifedipin GITS-nek kedvez. placebonak kedvez. Említésre méltó, hogy a nifedipin GITS 29%-kal csökkentette (p=0.015) az új manifeszt szívelégtelenség előfordulását. Ez egy nemvárt eredmény volt, melyet az isémiás epizódok hosszútávú csökkenése és ezen kívül a folyamatos csökkentett vérnyomás magyarázhat. A nifedipin GITS csoportban a stroke előfordulása 22%-kal csökkent (p=0.10). A növekvő vérnyomás és a stroke előfordulása között fennálló kapcsolat régóta bizonyított.1 Annak az oka, hogy ez az ACTION-ben nem érte el a statisztikai szignifikancia szintjét a járulékos vérnyomáscsökkenés nem elegendő mértéke, illetve a stroke szigorú definíciója volt. A nifedipin GITS kezeléssel együtt járt a refrakter angina előfordulásának csökkenő tendenciája a placebohoz hasonlítva (150 ill. 174, p=0.18). Ez fontos megfigyelés, mert a refrakter angina a betegség előrehaladásának jele, és instablisis angina vagy MI kialakulásának megnövekedett kockázata kapcsolódik hozzá. 1. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903–13.")
26
Alcsoport analysisek All patients Age <65 yrs (54%)
RR, 95% CI All patients Age <65 yrs (54%) 65 yrs (46%) p=0.4 History of MI No (49%) Yes (51%) p=0.2 blocker at entry No (20%) Yes (80%) p=0.5 ACE-i ARB at entry No (77%) Yes (23%) p=0.2 Blood pr. at entry <140/90 (48%) 140/90 (52%) p=0.02 Test for interaction: Favours nifedipine
 65 yrs (46%) p=0.4. History. of MI. No (49%) Yes (51%) p=0.2. blocker at entry. No (20%) Yes (80%) p=0.5. ACE-i ARB at entry. No (77%) Yes (23%) p=0.2. Blood pr. at entry. <140/90 (48%) 140/90 (52%) p=0.02. Test for interaction: Favours nifedipine.")
27
Angina pectorisos beteg gondozása. Noncardialis műtét
A beteg szedjen elégséges hatású (P<60/min) béta blockolót legalább egy héttel a műtét előtt kezdve Ha nem szedett, kezdjük el a műtét előtti este, lehetőleg intravénásan, és ha kell, folytassuk akár a műtét közben is a pl. metoprololt. (ACC guideline: Management of ischemic heart disease patient undergoing noncardiac surgery, 2001)
 béta blockolót legalább egy héttel a műtét előtt kezdve. Ha nem szedett, kezdjük el a műtét előtti este, lehetőleg intravénásan, és ha kell, folytassuk akár a műtét közben is a pl. metoprololt. (ACC guideline: Management of ischemic heart disease patient undergoing noncardiac surgery, 2001)")
30
Relative Risk Reduction = 53%*
Mortality Reduction After Acute Coronary Syndromes Following Lipid-Lowering Therapy (non-ST-elevation ACS patients, PURSUIT trial) Relative Risk Reduction = 53%* P=0.0002 *After adjusting for age, gender, hyperlipidemia, HF medications, baseline ECG Aronow HD, et al., JACC February 2000, Vol 35, Number 2:411A
 Relative Risk Reduction = 53%* P= *After adjusting for age, gender, hyperlipidemia, HF medications, baseline ECG. Aronow HD, et al., JACC February 2000, Vol 35, Number 2:411A.")
31
A coronarographia indikációi
Stabil effort angina (tünetes beteg) CCS II-IV a gyógyszerek ellenére Előbbiek szerint magas rizikó a provokációs teszten Hirtelen halál/sustained VT Kérdéses gyógyszerre javuló de meg nem szűnő angina olyan betegség, műtét, vagy foglalkozás, ahol a pontos diagnózis elkerülhetetlen
 CCS II-IV a gyógyszerek ellenére. Előbbiek szerint magas rizikó a provokációs teszten. Hirtelen halál/sustained VT. Kérdéses. gyógyszerre javuló de meg nem szűnő angina. olyan betegség, műtét, vagy foglalkozás, ahol a pontos diagnózis elkerülhetetlen.")
32
Revaszkularizáció és túlélés

33
Slide IV.1 The risk of morbidity and mortality is a major concern in patients with diabetes. By far the leading cause of death in people with diabetes is ischaemic heart disease. Approximately 75% of people with diabetes die of cardiovascular disease including stroke.26 After an MI, 40 to 50% of patients with diabetes die within 5 years.27,28

34
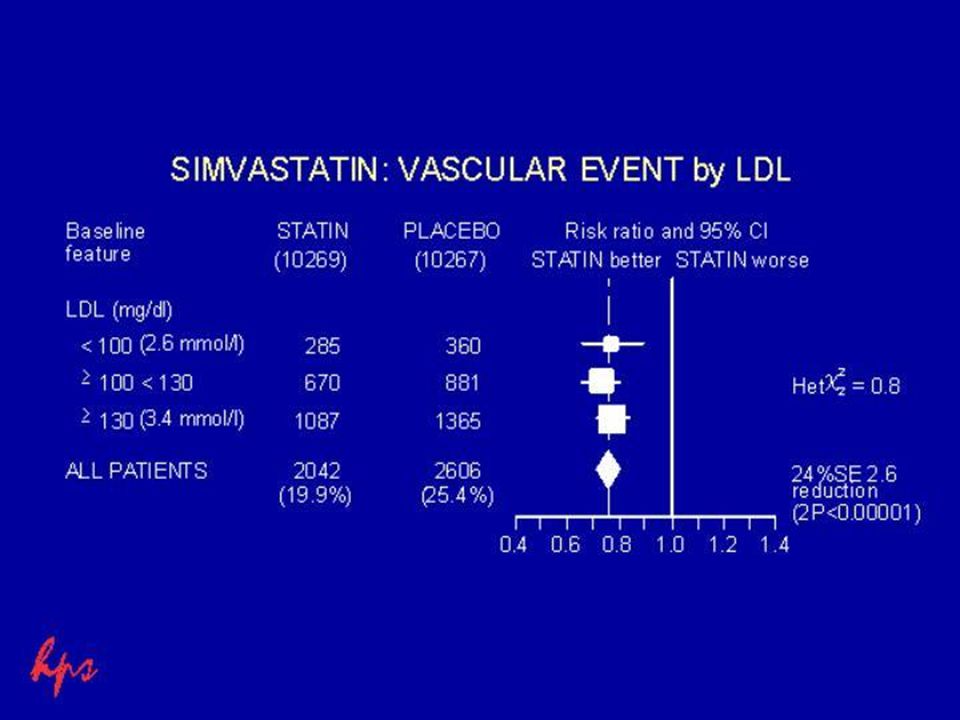
Slide IV.13 The post-hoc subgroup analysis of the Scandinavian Simvastatin Survival Study (4S) data in patients with diabetes (n=202) provides the first trial-based evidence that cholesterol lowering improves the prognosis of diabetic patients with CHD.34 As shown on this slide, simvastatin significantly reduced the risk of coronary death and nonfatal MIs in diabetic patients with previous MI and/or angina pectoris by 55% (P=0.002). In non-diabetics, there was a 32% reduction in risk (P=0.0001). Treatment with simvastatin reduced the risk of coronary death/MI in patients with diabetes to a level similar to that in non-diabetics. 34
 data in patients with diabetes (n=202) provides the first trial-based evidence that cholesterol lowering improves the prognosis of diabetic patients with CHD.34. As shown on this slide, simvastatin significantly reduced the risk of coronary death and nonfatal MIs in diabetic patients with previous MI and/or angina pectoris by 55% (P=0.002). In non-diabetics, there was a 32% reduction in risk (P=0.0001). Treatment with simvastatin reduced the risk of coronary death/MI in patients with diabetes to a level similar to that in non-diabetics. 34.")
35
SPECIAL GROUPS COCAINE
Class I 1. NTG and oral Ca2+ blocker for pts with ST deviation that accompanies ischemic chest discomfort. 2. Immediate coronary arteriography in pts with ST elevation after NTG and Ca2+ blocker; thrombolysis if a thrombus is detected.

39
PCI - stent

41
Kibocsátási gyógyszerek NSTE ACS
IIa IIb III Aspirin, ha nem kontraindikált Clopidogrel, ha aspirin kontraindikált Aspirin + Clopidogrel, 9 hónapig Béta blockoló statin ACE Inhibitor: szívelégt., EF < 40%, DM, hypertonia None

42
Atherothrombosis a civilizált világ vezető haláloka
Pulmonary Disease 6.3 Injuries 9 AIDS 9.7 Cancer 12.6 Infectious Disease 19.3 Atherothrombosis is the underlying condition that results in events leading to myocardial infarction, ischemic stroke, and vascular death. As such, the leading cause of death of the estimated 55,694,000 people worldwide who died in 2000 was atherothrombosis, manifested as cardiovascular disease, ischemic heart disease and stroke (52% of deaths). Other main causes of death were AIDS (5%) pulmonary disease (6%) injuries (9%) cancer (12%) violent death (12%) infectious diseases (19%) Atherothrombosis (29%) Atherothrombosis* 22.3 5 10 15 20 25 30 Causes of Mortality (%) 1 The World Health Report Geneva. WHO References The World Health Report Geneva: WHO; 2001.
. Other main causes of death were. AIDS (5%) pulmonary disease (6%) injuries (9%) cancer (12%) violent death (12%) infectious diseases (19%) Atherothrombosis (29%) Atherothrombosis* Causes of Mortality (%) 1 The World Health Report Geneva. WHO References. The World Health Report Geneva: WHO;")
43
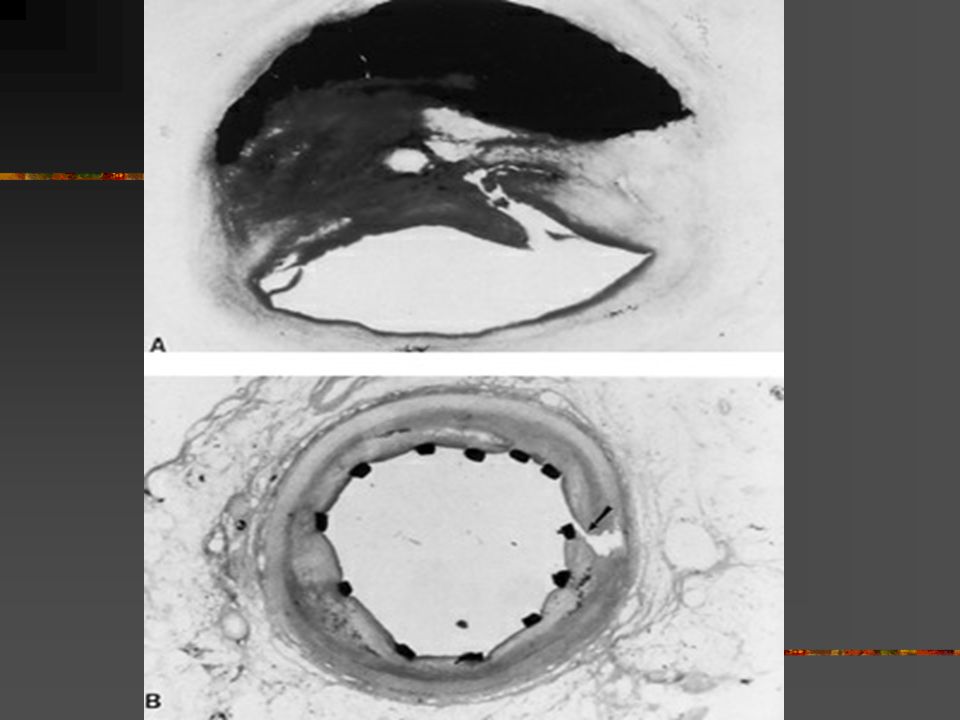
In this slide, the lipid core is separated from the lumen by a thin fibrous cap.
Courtesy of Professor Michael J. Davies.

44
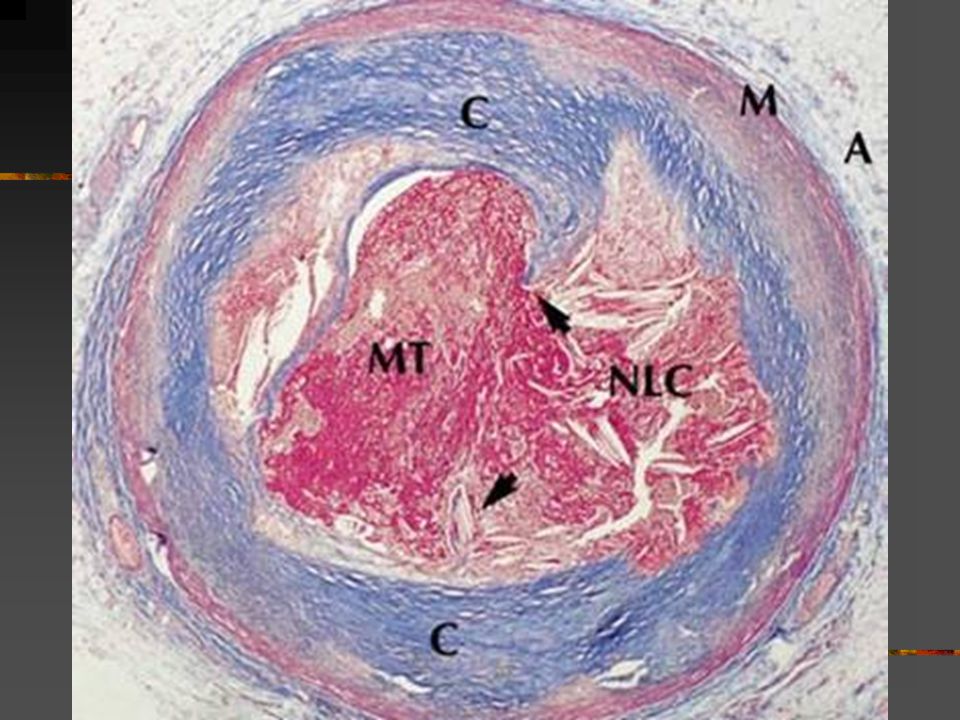
In this slide, cap disruption has precipitated thrombosis.
Courtesy of Professor Michael J. Davies.

46
Evidence of Multiple “Vulnerable” Plaques in ACS
plaques detected in non-culprit segments 1-7 Asakura M, et al. J Am Coll Cardiol. 2001;37:1284 Multiple “vulnerable” plaques detected in non-culprit segments 10-12 Evidence of Multiple “Vulnerable” Plaques in ACS Angiographic & angioscopic images in 58-year-old man with anterior myocardial infarction Culprit lesion (#8) detected with thrombus (red) The formation of vulnerable plaques is part of a pan-coronary process. The number of yellow plaques and thrombis in the left anterior descending coronary artery, left circumflex artery, and the right coronary artery were evaluated angiographically in 32 patients undergoing catherization 1 month after myocardial infarction (MI). The mean number of yellow plaques detected in a coronary artery, excluding the culprit lesion, was 3.2 ± 1.7. Yellow plaques were equally prevalent in the infarct-related and non–infarct-related coronary arteries (3.7 ± 1.6 vs 3.4 ± 1.8 plaques per artery, P=NS). Angioscopic images from a 58-year old man who had an anterior wall MI reveal a culprit lesion in numbers 8 and 9, along with a thrombus. Multiple other vulnerable yellow plaques were detected throughout the coronary vasculature (1-7 and 10-12). Vulnerable plaques exist in the culprit lesion and in the nonculprit segments. Treatment should be designed to prevent future ischemic events due to the culprit or nonculprit lesions. References 1 Asakura M, Ueda Y, Yamaguchi O, et al. Extensive development of vulnerable plaques as a pan-coronary process in patients with myocardial infarction: an angioscopic study. J Am Coll Cardiol. 2001;37: ACS, acute coronary syndrome. Asakura M, et al. J Am Coll Cardiol. 2001;37: (with permission)
 detected with. thrombus (red) The formation of vulnerable plaques is part of a pan-coronary process. The number of yellow plaques and thrombis in the left anterior descending coronary artery, left circumflex artery, and the right coronary artery were evaluated angiographically in 32 patients undergoing catherization 1 month after myocardial infarction (MI). The mean number of yellow plaques detected in a coronary artery, excluding the culprit lesion, was 3.2 ± 1.7. Yellow plaques were equally prevalent in the infarct-related and non–infarct-related coronary arteries (3.7 ± 1.6 vs 3.4 ± 1.8 plaques per artery, P=NS). Angioscopic images from a 58-year old man who had an anterior wall MI reveal a culprit lesion in numbers 8 and 9, along with a thrombus. Multiple other vulnerable yellow plaques were detected throughout the coronary vasculature (1-7 and 10-12). Vulnerable plaques exist in the culprit lesion and in the nonculprit segments. Treatment should be designed to prevent future ischemic events due to the culprit or nonculprit lesions. References. 1 Asakura M, Ueda Y, Yamaguchi O, et al. Extensive development of vulnerable plaques as a pan-coronary process in patients with myocardial infarction: an angioscopic study. J Am Coll Cardiol. 2001;37: ACS, acute coronary syndrome. Asakura M, et al. J Am Coll Cardiol. 2001;37: (with permission)")
47
Szimultán megjelenő nonculprit plaque rupturák száma (a betegek %-ában)
Rioufol Circulation 2002; 106: 804

48
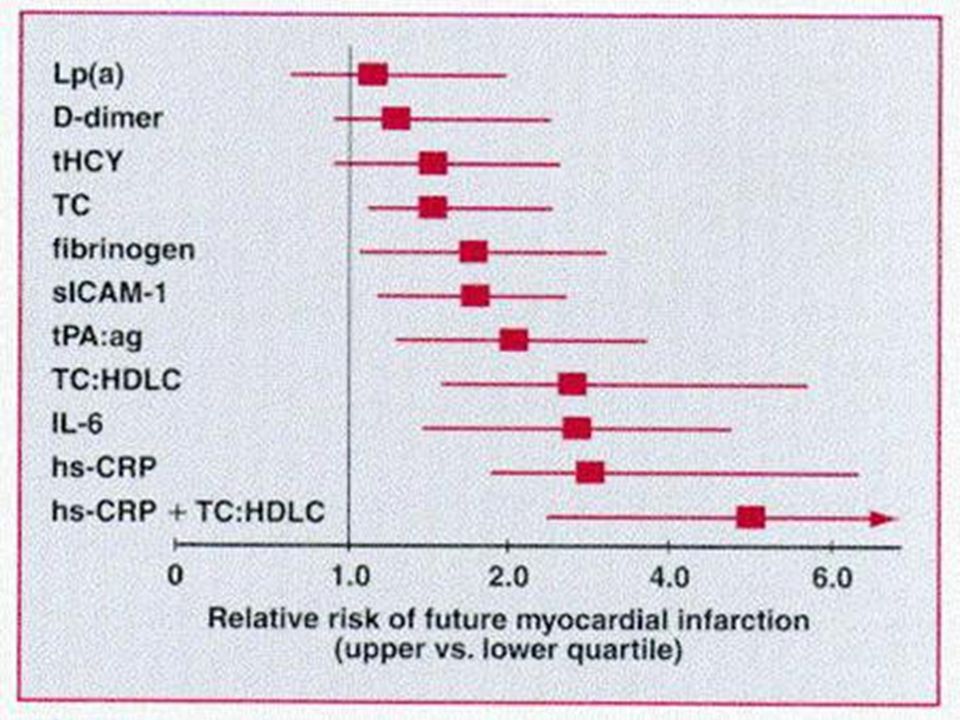
CRP és rizikó CRP független cardiovascularis rizikófaktor
Statinok és az aspirin képesek a gyulladás által okozott többletrizikó neutralizálására A gyulladásos markernek tartott CRP önmaga is mediátorként viselkedik és károsítja az érrendszert

49
Aspirin, gyulladás és cardiovascularis rizikó
AMI rizikó CRP quartilisok Ridker NEJM 1997; 336: 973

50
Pravastatin, gyulladás és cardiovascularis rizikó
RR Ridker Circulation 1998; 98: 839

52
Thrombocytagátlók támadáspontjai
ADP dipyridamole Clopidogrel ticlopidine HCl ADP phosphodiesterase ADP cAMP collagen thrombin TXA2 Activation (fibrinogen receptor) GP IIb/IIIa The mechanism of action of clopidogrel is similar to that of ticlopidine but different from that of aspirin.[1] Both clopidogrel and ticlopidine require biotransformation for their pharmacologic activity. Clopidogrel is a potent, noncompetitive inhibitor of ADP-induced platelet aggregation. Clopidogrel inhibits the binding of ADP to platelet membrane receptors. The effect of clopidogrel on ADP binding is irreversible[2] and lasts for the duration of platelet life, about 7 to 10 days. The inhibition is also specific and does not significantly affect cyclooxygenase or arachidonic acid metabolism.[1] Both low- and high-affinity ADP receptors are present on platelets, and the active metabolite of clopidogrel binds to the low-affinity receptors.[1] ADP binding to this site is necessary for activation of the GP IIb/IIIa receptor, which is the binding site for fibrinogen. Fibrinogen links different platelets together to form the platelet aggregate.[3] Clopidogrel thus ultimately inhibits the activation of the GP IIb/IIIa receptor and its binding with fibrinogen.[3] Aspirin inhibits the cyclooxygenase enzyme, preventing the production of prostaglandin and thromboxane A2 (TXA2) from arachidonic acid.[3] TXA2 activates the GP IIb/IIIa binding site on the platelet, allowing fibrinogen to bind. Aspirin also exerts its effects on other parts of the body system.[3] Paradoxically, aspirin blocks synthesis of prostacyclin by endothelial cells, resulting in an effect that promotes platelet aggregation.[3] Dipyridamole has been suggested to act as an antiplatelet drug by several possible mechanisms. It directly stimulates prostacyclin synthesis, potentiates the platelet inhibitory actions of prostacyclin, and inhibits phosphodiesterase to raise platelet cyclic AMP (cAMP) levels. However, these effects may not occur at therapeutic levels of the drug; hence the mechanism of action of dipyridamole remains to be elucidated.[3] Schrör K. The basic pharmacology of ticlopidine and clopidogrel. Platelets. 1993;4: Plavix® (clopidogrel bisulfate) Prescribing Information. Schafer AI. Antiplatelet therapy. Am J Med. 1996;101: COX aspirin TXA2 ADP = adenosine diphosphate, TXA2 = thromboxane A2, COX = cyclooxygenase. Schafer AI. Am J Med. 1996;101:
 GP IIb/IIIa. The mechanism of action of clopidogrel is similar to that of ticlopidine but different from that of aspirin.[1] Both clopidogrel and ticlopidine require biotransformation for their pharmacologic activity. Clopidogrel is a potent, noncompetitive inhibitor of ADP-induced platelet aggregation. Clopidogrel inhibits the binding of ADP to platelet membrane receptors. The effect of clopidogrel on ADP binding is irreversible[2] and lasts for the duration of platelet life, about 7 to 10 days. The inhibition is also specific and does not significantly affect cyclooxygenase or arachidonic acid metabolism.[1] Both low- and high-affinity ADP receptors are present on platelets, and the active metabolite of clopidogrel binds to the low-affinity receptors.[1] ADP binding to this site is necessary for activation of the GP IIb/IIIa receptor, which is the binding site for fibrinogen. Fibrinogen links different platelets together to form the platelet aggregate.[3] Clopidogrel thus ultimately inhibits the activation of the GP IIb/IIIa receptor and its binding with fibrinogen.[3] Aspirin inhibits the cyclooxygenase enzyme, preventing the production of prostaglandin and thromboxane A2 (TXA2) from arachidonic acid.[3] TXA2 activates the GP IIb/IIIa binding site on the platelet, allowing fibrinogen to bind. Aspirin also exerts its effects on other parts of the body system.[3] Paradoxically, aspirin blocks synthesis of prostacyclin by endothelial cells, resulting in an effect that promotes platelet aggregation.[3] Dipyridamole has been suggested to act as an antiplatelet drug by several possible mechanisms. It directly stimulates prostacyclin synthesis, potentiates the platelet inhibitory actions of prostacyclin, and inhibits phosphodiesterase to raise platelet cyclic AMP (cAMP) levels. However, these effects may not occur at therapeutic levels of the drug; hence the mechanism of action of dipyridamole remains to be elucidated.[3] Schrör K. The basic pharmacology of ticlopidine and clopidogrel. Platelets. 1993;4: Plavix® (clopidogrel bisulfate) Prescribing Information. Schafer AI. Antiplatelet therapy. Am J Med. 1996;101: COX. aspirin. TXA2. ADP = adenosine diphosphate, TXA2 = thromboxane A2, COX = cyclooxygenase. Schafer AI. Am J Med. 1996;101:")
53
A thrombocytagátló kezelés hatása a cardiovascularis eseményekre.
195 tanulmány, beteg Antithrombotic Trialists’ Collaboration BMJ 2002; 324:

54
Az aspirin dózisa és a vascularis történések előfordulása
Aspirin Dosis # Trials OR* (%) Odds Ratio 500–1500 mg 160–325 mg 75–150 mg <75 mg Any aspirin The Antithrombotic Trialists’ Collaboration compared data from 65 aspirin trials to examine the effects of aspirin dose on vascular events in high-risk patients (in some trials, the doses of aspirin used were in more than one of the comparisons).[1] Serious vascular events (the primary measure of outcome) included nonfatal MI, nonfatal stroke, death from vascular causes, and death from unknown causes. They found that all doses of aspirin studied reduced the risk for vascular events. The greatest number of trials (34) examined high aspirin doses (500 mg to 1500 mg) and revealed a proportional reduction in vascular events of 19%. Aspirin doses of 160 mg to 325 mg were associated with a 26% proportional reduction in vascular events, whereas 75 mg to 150 mg and <75 mg were associated with reductions of 32% and 13%, respectively. Antithrombotic Trialists’ collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324:71-86. 0.5 1.0 1.5 2.0 ASA better ASA worse *Odds reduction Treatment effect P < Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:71-86.
 Odds Ratio. 500–1500 mg –325 mg –150 mg <75 mg Any aspirin The Antithrombotic Trialists’ Collaboration compared data from 65 aspirin trials to examine the effects of aspirin dose on vascular events in high-risk patients (in some trials, the doses of aspirin used were in more than one of the comparisons).[1] Serious vascular events (the primary measure of outcome) included nonfatal MI, nonfatal stroke, death from vascular causes, and death from unknown causes. They found that all doses of aspirin studied reduced the risk for vascular events. The greatest number of trials (34) examined high aspirin doses (500 mg to 1500 mg) and revealed a proportional reduction in vascular events of 19%. Aspirin doses of 160 mg to 325 mg were associated with a 26% proportional reduction in vascular events, whereas 75 mg to 150 mg and <75 mg were associated with reductions of 32% and 13%, respectively. Antithrombotic Trialists’ collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324: ASA better. ASA worse. *Odds reduction. Treatment effect P < Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:")
55
ASA dózis és major vérzés
CURE Study ASA dózis és major vérzés Clopidogrel + ASA* Placebo + ASA* ASA Dose <100 mg 2.6% % 100–200 mg 3.5% % >200 mg 4.9% % Definition of major bleeding[1]: Life-threatening bleeding, which was defined as fatal or leading to one of the following: intracranial hemorrhage, drop in hemoglobin of 5 g/dL, substantial hypotension requiring inotropic therapy, surgical intervention, or transfusion of 4 or more units of blood. Other major bleeding was defined as substantially disabling bleeding, intraocular bleeding leading to the loss of vision, or bleeding necessitating the transfusion of 2 to 3 units of blood. Major bleeding episodes were primarily gastrointestinal hemorrhages or bleeding at site of arterial puncture.[2] The incidence of major bleeding increased with aspirin (ASA) dose in both treatment groups, with the highest incidence among patients receiving more than 200 mg of ASA.[1] The CURE trial was not powered to detect differences in bleeding rates by ASA dose. However, after adjusting for risk factors for bleeding (ie, age, gender, serum creatinine, elevated enzymes, ST depression at baseline, weight, and BMI), the odds ratio for major bleeding for ASA 325 mg vs ASA 75 mg was 2.07 (P = ).[3] Plavix® (clopidogrel sulfate) Prescribing Information. The CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345: Data on file, Sanofi-Synthelabo. *Other standard therapies were used as appropriate. PLAVIX Prescribing Information.
 dose in both treatment groups, with the highest incidence among patients receiving more than 200 mg of ASA.[1] The CURE trial was not powered to detect differences in bleeding rates by ASA dose. However, after adjusting for risk factors for bleeding (ie, age, gender, serum creatinine, elevated enzymes, ST depression at baseline, weight, and BMI), the odds ratio for major bleeding for ASA 325 mg vs ASA 75 mg was 2.07 (P = ).[3] Plavix® (clopidogrel sulfate) Prescribing Information. The CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345: Data on file, Sanofi-Synthelabo. *Other standard therapies were used as appropriate. PLAVIX Prescribing Information.")
56
Chan et al N Engl J Med 2005:352; 238-44.

57
A thrombocytagátló profilakszis hatékonysága elsősorban cardiovascularis betegség súlyosságától függ
Patrono, C. et al. Chest 2004;126:234S-264S

58
Abszolut benefit és vérzéses kockázat primer prevencióban. ASA
Patrono, C. et al. Chest 2004;126:234S-264S

59
1,000 személy/év aspirin kezelése során megelőzött maior cv. esemény
Diagnózis Benefit* Risk Még nem beteg férfi, cv. kockázattal 1–2 Essentialis hypertonia Chronicus stabil angina 10 Korábbi MI 20 Instabil angina 50

60
Primer prevenció Legalább közepes mértékű cv. rizikó (10 éves kockázat> 10%), 75 to 162 mg/d aspirin javasolt, mely hatékonyabb, mint a kezelés nélkül hagyás vagy a kumarin (Grade 2A). ACCP VII. Consensus Chest 2004 Sep
, 75 to 162 mg/d aspirin javasolt, mely hatékonyabb, mint a kezelés nélkül hagyás vagy a kumarin (Grade 2A). ACCP VII. Consensus Chest 2004 Sep.")
61
Krónikus coronaria betegség
Krónikus stabil coronariabetegnek mg aspirin javasolt (Grade 1A). Életfogytig (Grade 2C). Azoknak, akiknél magas a myocardialis infarctus kockázata, 75 mg clopidogrel és aspirin együttes adása javasolt (Grade 2C). ACCP VII. Consensus Chest 2004 Sep
. Életfogytig (Grade 2C). Azoknak, akiknél magas a myocardialis infarctus kockázata, 75 mg clopidogrel és aspirin együttes adása javasolt (Grade 2C). ACCP VII. Consensus Chest 2004 Sep.")
62
Aspirin PCI esetén Minden betegnek ( mg telítő és fenntartó napi oralis dózis) Minimum 30 perccel a PCI előtt beadva Élethosszig Költség: 4 cent Lange, Hillis: N Engl J Med 2004; 350: 3

63
IAP/NSTEMI Aspirin Cairns Lewis Theroux Wallentin összes 1.0 2.0
This slide of five randomized trials show there is a 25-30% reduction in the risk of death or MI when comparing aspirin vs placebo in patients presenting with acute coronary syndrome. Aspirin 1.0 Placebo 2.0 Relativ kockázat — halál vagy AMI

64
Az acetylszalicilsav cyclooxygenáz- gátlásának molekuláris mechanizmusa
COX-1 COX-2 O CH C 3 arachidonsav Ser O O O C Ser CH 3 Arachidonsav Allen,K.N után módosÍtott.: Nature Med. 1(9), (1995)
, (1995)")
65
Az acetylszalicilsav rezisztencia (egyik) molekuláris mechanizmusa
COX-1 COX-2 Ibuprofen++ Diclofenac +- Coxib- O CH C 3 arachidonsav Ser O Ser NSAID ASA Arachidonsav F Catella-Lawson NEJM 2001 dec 20 Allen,K.N után módosÍtott.: Nature Med. 1(9), (1995)
, (1995)")
66
RR:1·93 (1·30-2·87) P=0,0011 Risk of all-cause and cardiovascular mortality in patients with cardiovascular disease Lancet 2003; 361:

67
Fiziológiás antagonizmus a prosztacyclin és thromboxán között
Arachidonsav Cyclooxygenáz Endoperoxidok PGG2 PGH2 Thrombocyta- aktiválás Értónus simaizomsejtek proliferációja PGI2 gátlás TXA2 aktiválás Érendothel Thrombocyta

68
Szelektív prostacyclin gátlás
COX2 inhibitorok (coxibok) szelektíven gátolják a prostacyclin szintézist, míg a TXA2 termelődés nem gátolt Prostacyclin receptorokkal nem rendelkező egerek carotist thrombosist kaptak, míg prostacyclin és TXA2 receptor-hiányos egerek nem. A coxibok nem képesek megelőzni, vagy éppen triggerelik az atherothrombosist Cheng Y: Role of prostacyclin in the cardiovascular response to TXA2. Science 2002; 296:539 Bombardier Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen with rheumatoid arthritis. N Engl J Med 2000; 343: 1520
 szelektíven gátolják a prostacyclin szintézist, míg a TXA2 termelődés nem gátolt. Prostacyclin receptorokkal nem rendelkező egerek carotist thrombosist kaptak, míg prostacyclin és TXA2 receptor-hiányos egerek nem. A coxibok nem képesek megelőzni, vagy éppen triggerelik az atherothrombosist. Cheng Y: Role of prostacyclin in the cardiovascular response to TXA2. Science 2002; 296:539. Bombardier Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen with rheumatoid arthritis. N Engl J Med 2000; 343:")
69
Thrombosis/endothel A thrombocytában a COX1 hatás a domináns, aspirin gátol, NSAID-ok kevésbé, coxibok nem gátolják a TxA2-t Az érfalban a PGI2 termelődését minden COX gátló (aspirin, NSAID, coxib) gátolja COX 2 gátlásnál az endothel védőfunctioja elvileg gyengített, míg a thrombocyták nem gátoltak és TXA-2-t szintetizálnak: atherothrombotikus rizikófokozódás?
 gátolja. COX 2 gátlásnál az endothel védőfunctioja elvileg gyengített, míg a thrombocyták nem gátoltak és TXA-2-t szintetizálnak: atherothrombotikus rizikófokozódás")
70
Thrombotikus rizikó Atherothrombosis, atherosclerosis szempontjából veszélyeztetett betegen a nonselectiv COX inhibitor (főként a naproxen) jobb választás, mint a coxib. Nem bizonyított, hogy ilyen esetben kell-e kombinálni aspirinnel (GI versus CV risk) A coxib és aspirin kombináció teljességgel értelmetlen és drága.
 jobb választás, mint a coxib. Nem bizonyított, hogy ilyen esetben kell-e kombinálni aspirinnel (GI versus CV risk) A coxib és aspirin kombináció teljességgel értelmetlen és drága.")
71
Cardioprotectio vs. gastroprotectio
Ha a betegnek cardialis okból aspirint kell szednie, nem érdemes coxibot adni, mert a GI mellékhatások az aszpirin miatt fognak megjelenni (lásd CLASS) Ha COX2 selectiv gyógyszert adunk, nem lesz cardioprotectio, még annyi sem, mint a nonselectiv NSAID-oknál (lásd VIGOR) Cardiológus-rheumatológus-gastroenterologus = jó háziorvos M. Boers, Lancet, 2001, 357: 1222
 Ha COX2 selectiv gyógyszert adunk, nem lesz cardioprotectio, még annyi sem, mint a nonselectiv NSAID-oknál (lásd VIGOR) Cardiológus-rheumatológus-gastroenterologus = jó háziorvos. M. Boers, Lancet, 2001, 357:")
72
Kibocsátási gyógyszerek NSTE ACS
IIa IIb III Aspirin, ha nem kontraindikált Clopidogrel, ha aspirin kontraindikált Aspirin + Clopidogrel, 9 hónapig Béta blockoló statin ACE Inhibitor: szívelégt., EF < 40%, DM, hypertonia None

73
N: 3630 Hurlen NEJM 2002 szept 26

74
Perioperatív ASA kezelés coronaria bypassműtét során
70 centrumban 5065 beteg, prospektív adatgyűjtés Halálozás: ASA elkezdve az első 48 órán belül: 1,3%, ASA nélkül: 4,0 % (p<0,001) Periop AMI: ASA az első 48 órán belül: 2,8 % vs 5,4% (p<0,001) 1,3 vs 2,6 % stroke (p=0,01) 0,9 vs 3,4% veseelégtelenség (p<0,001) 0,3 vs 0,8% bélinfarctus (p=0,01) Maior vérzés: NS From Taboo to New Standard of Care Mangano NEJM 2002 okt 24
 Periop AMI: ASA az első 48 órán belül: 2,8 % vs 5,4% (p<0,001) 1,3 vs 2,6 % stroke (p=0,01) 0,9 vs 3,4% veseelégtelenség (p<0,001) 0,3 vs 0,8% bélinfarctus (p=0,01) Maior vérzés: NS. From Taboo to New Standard of Care. Mangano NEJM 2002 okt 24.")
76
CABG Minden coronaria beteg szedjen mg aspirint (Grade 1A). A CABG műtöttek is kapjanak aspirint, (Grade 1A) lehetőleg 6 órával a műtét után. Ha a vérzés ezt nem teszi lehetővé, akkor az első lehetséges időpontban (Grade 1C). ACCP 2004 sept
 lehetőleg 6 órával a műtét után Ha a vérzés ezt nem teszi lehetővé, akkor az első lehetséges időpontban (Grade 1C). ACCP 2004 sept.")
77
AMI és ACS után STE vagy NSTE ACS után:
Aspirin kezdetben mg, majd mg/d (Grade 1A). Magas vérzéses kockázat vagy korábbi aspirin okozta vérzés esetén kisebb dózisú (<=100 mg) aspirin (Grade 1C+). Aspirin intolerancia esetén tartósan adott clopidogrel: 75 mg/d (Grade 1A). ACCP VII. Consensus Chest 2004 Sep
. Magas vérzéses kockázat vagy korábbi aspirin okozta vérzés esetén kisebb dózisú (<=100 mg) aspirin (Grade 1C+). Aspirin intolerancia esetén tartósan adott clopidogrel: 75 mg/d (Grade 1A). ACCP VII. Consensus Chest 2004 Sep.")
78
Clopidogrel vs ASA hatékonysága a cardiovascularis eseményekre
8.7%* Évenkénti események 16 RR ASA 5.83% 12 (N=19,185) Összes esemény (%) 8 5.32% Clopidogrel SLIDE 16 Clopidogrel Efficacy vs. ASA in preventing MI, ischemic stroke, or vascular death Clopidogrel versus ASA in Patients at Risk of Ischemic Events (CAPRIE) is an international comparative clinical trial of the efficacy of clopidogrel and ASA performed in 19,185 patients at increased risk of atherosclerosis, documented by recent stroke or myocardial infarction or established peripheral artery disease. Patients were enrolled over 3 years and followed up for 1 to 3 years (mean follow-up 1.9 years). The measured outcomes of the CAPRIE study were ischemic stroke, myocardial infarction, or vascular death (CAPRIE Steering Committee 1996). A total of 939 patients in the clopidogrel group and 1021 patients in the ASA group experienced one of the outcome events (5.3% versus 5.8%). The overall relative risk reduction with clopidogrel for an outcome event was 8.7%, over and above ASA, a statistically significant finding (p = 0.043) (CAPRIE Steering Committee 1996). The CAPRIE study demonstrated that long-term administration of clopidogrel to patients with atherosclerotic vascular disease is more effective than ASA in reducing the combined risk of ischemic stroke (non-fatal or fatal), myocardial infarction (non-fatal or fatal) or other vascular death (CAPRIE Steering Committee 1996). CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus ASA in patients at risk of ischemic events (CAPRIE). Lancet 1996;348: 4 P = 0.043 3 6 9 12 15 18 21 24 27 30 33 36 Hónapok *ITT analysis. CAPRIE Steering Committee. Lancet 1996;348: 25
 Összes esemény (%) % Clopidogrel. SLIDE 16 Clopidogrel Efficacy vs. ASA in preventing MI, ischemic stroke, or vascular death. Clopidogrel versus ASA in Patients at Risk of Ischemic Events (CAPRIE) is an international comparative clinical trial of the efficacy of clopidogrel and ASA performed in 19,185 patients at increased risk of atherosclerosis, documented by recent stroke or myocardial infarction or established peripheral artery disease. Patients were enrolled over 3 years and followed up for 1 to 3 years (mean follow-up 1.9 years). The measured outcomes of the CAPRIE study were ischemic stroke, myocardial infarction, or vascular death (CAPRIE Steering Committee 1996). A total of 939 patients in the clopidogrel group and 1021 patients in the ASA group experienced one of the outcome events (5.3% versus 5.8%). The overall relative risk reduction with clopidogrel for an outcome event was 8.7%, over and above ASA, a statistically significant finding (p = 0.043) (CAPRIE Steering Committee 1996). The CAPRIE study demonstrated that long-term administration of clopidogrel to patients with atherosclerotic vascular disease is more effective than ASA in reducing the combined risk of ischemic stroke (non-fatal or fatal), myocardial infarction (non-fatal or fatal) or other vascular death (CAPRIE Steering Committee 1996). CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus ASA in patients at risk of ischemic events (CAPRIE). Lancet 1996;348: P = Hónapok. *ITT analysis. CAPRIE Steering Committee. Lancet 1996;348:")
79
Globális eredmény: CV halál/MI PCI-CURE
0.0 0.05 0.10 0.15 40 100 200 300 400 10 A B PCI utáni napok Kumulativ kockázat RR 0.69 95% CI P=0.002 ASA+Clopidogrel ASA A=median idő PCI-ig B=30 nap PCIután

80
Clopidogrel és statinok metabolizmusa
észteráz prava Karboxilsav clopi metabolit CYP 3A4 atorva, simva, ceriva CYP 2C9 fluva Aktív clopi metabolit Inaktív clopi metabolit

81
Clopidogrel + statin interakció? GRACE registry
% N:7412 ASA+clopi ASA+clopi+statin MJ LIM, RH Mehta ACC 2003;

82
(J Am Coll Cardiol 2003;41:969 –73) N: 700, randomized 75 mg clopidogrel or 500 mg ticlopidine for four weeks after stent impl.

83
30-Day Major Adverse Cardiac Events
Efficacy of Clopidogrel or Ticlopidine in Reducing Coronary Events After Stenting 30-Day Major Adverse Cardiac Events Trial N Odds Ratio & 95% CI Clopid. (%) Ticl. (%) CLASSICS 1020 1.3 0.9 TOPPS 1016 2.6 3.5 Müller 700 3.1 1.7 CCF 2369 5.7 8.9 Lenox Hill 2565 2.4 3.8 Mayo 2827 0.6 1.6 N. Memorial 1378 0.8 2.2 S. Illinois 875 2.1 1.4 Wash. Hosp. 844 2.0 0.5 Wessex -361 3.4 5.2 Overall 13,955 OR=.73, P=.003 2.0 3.9 0.1 Clopidogrel Better 1 Ticlopidine Better 10 CLASSICS, Clopidogrel Aspirin Stent Intervention Coopoerative Study. Bhatt DL, et al. J Am Coll Cardiol. 2002;39:9-14. (with permission)
 Ticl. (%) CLASSICS TOPPS Müller CCF Lenox Hill Mayo N. Memorial S. Illinois Wash. Hosp Wessex Overall. 13,955. OR=.73, P= Clopidogrel Better. 1. Ticlopidine Better. 10. CLASSICS, Clopidogrel Aspirin Stent Intervention Coopoerative Study. Bhatt DL, et al. J Am Coll Cardiol. 2002;39:9-14. (with permission)")
84
Clopidogrel PCI esetén
Minden beteg kapjon mg telítő adagot ideális esetben >4 órával a PCI előtt, majd 75 mg napi fenntartó adagot A kezelés tartama : 9-12 hónap Költsége: 4 USD naponta Alacsony és közepes rizikó esetén az előkezelés kiváltja a Gp IIb/IIIa blokkoló adását Lange, Hillis: N Engl J Med 2004; 350: 3

85
NSTE ACS Thienopyridinek
Aspirin allergia/intolerancia esetén azonnali clopidogrel, 300 mg oralis bolus, majd 75 mg/d tartósan (Grade 1A). ACCP VII. Consensus Chest 2004 Sep
. ACCP VII. Consensus Chest 2004 Sep.")
86
NSTE ACS Ha sürgős coronarographia nincs tervezve, illetve acut CABG műtét 5 napon belül nem várható, azonnali clopidogrel kezelés javasolt (300 mg, majd 75 mg/d 9-12 hónapig), aspirinnel együtt (Grade 1A). ACCP VII. Consensus Chest 2004 Sep
, aspirinnel együtt (Grade 1A). ACCP VII. Consensus Chest 2004 Sep.")
87
NSTE ACS Ha 24 órán belül coronarographiát tervezünk, halasszuk a clopidogrel elkezdését a coronaria anatomia megismerése utánra (Grade 2A). Clopidogrel szedőknél a CABG műtét előtt 5 nappal hagyjuk ki a gyógyszert (Grade 2A). ACCP VII. Consensus Chest 2004 Sep
. ACCP VII. Consensus Chest 2004 Sep.")
88
STEMI prehosp. 162-325 mg aspirin elrágása az első ellátáskor (I)
Aspirin tanácsolása már a telefonriasztáskor (IIa) Legyen helyszini 12 elvezetéses EKG ACC AHA AMI ajánlás 2004
 Legyen helyszini 12 elvezetéses EKG. ACC AHA AMI ajánlás")
89
STEMI PPCI clopidogrel
CABG előtt lehetőleg 5-7 napig szünet Stent esetén ideálisan 12 hónapig clopi De legkevesebb: 1 hónap nem DES 3 hónap sirolimus DES 6 hónap paclitaxel DES esetén Minden ajánlás I-es szintű ACC AHA AMI ajánlás 2004

90
STEMI után kumarin ASA allergia stent nélkül, ilyenkor vagy kumarin, vagy clopidogrel (INR ) ASA allergia stenttel, ilyenkor kumarin clopidogrellel együtt (INR ) P. fibr BK thrombus (INR )(eddig I) Secunder prevencióban, különösen, ha BK dysfunctio és kiterjedt falmozgászavar van (IIa) ACC AHA AMI ajánlás 2004
 P. fibr BK thrombus (INR )(eddig I) Secunder prevencióban, különösen, ha BK dysfunctio és kiterjedt falmozgászavar van (IIa) ACC AHA AMI ajánlás")
91
A thrombocytagátló kezelés hatása a cardiovasc. eseményekre
195 tanulmány, beteg 7705 Antithrombotic Trialists’ Collaboration BMJ 2002; 324:

92
Aspirin rezisztencia hatása a cardiovascularis eseményekre
Odds ratio aspirin ThromboxanB2 ng/mmol creat. Thromboxan B2 Eikelboom Circulation 2002;105: 1650

93
Nyitott kérdés Drug compliance (arachidonsavval feltárható)
Relationship of laboratory measurements and (other) clinical endpoints? Combination therapy or drug change? Drug dose?
 clinical endpoints Combination therapy or drug change Drug dose")
94
Thrombocyta aggregáció gátlása
Slide I.13 The combined effect of platelet adhesion and platelet recruitment by agonists such as thrombin exposes the integrin platelet glycoprotein IIb/IIIa receptor,13,15 which is present in as many as 50,000 copies on the surface of each platelet.32 Like other members of the integrin family, platelet glycoprotein IIb/IIIa receptors are specific for the amino-acid sequence arginine-glycine-aspartic acid, or RGD.32 Thus, adhesive proteins, such as fibrinogen, that contain an RGD sequence can bind to the glycoprotein IIb/IIIa receptor.23 Indeed, the primary function of this receptor is to provide a binding site for fibrinogen. Activated platelets form aggregates by cross-linking through fibrinogen's multiple glycoprotein IIb/IIIa receptor binding sites.23 Once platelets begin cross-linking with fibrinogen, they rapidly join together into doublets, triplets, and multiple groups. These aggregates enlarge at the site of vessel damage.33 Following atherosclerotic plaque rupture, large platelet aggregates can potentially lead to a critical occlusion of the diseased vessel.16 Elucidation of the pathophysiology of thrombus formation has shown that the binding of fibrinogen to the platelet glycoprotein IIb/IIIa receptor is the final, obligatory pathway to platelet aggregation.15 By preventing the binding or interaction of the receptor with fibrinogen, glycoprotein IIb/IIIa receptor antagonists help prevent platelet aggregation and subsequent thrombus formation.15

96
Gp IIb/IIIa bénítók hatása acut coronaria syndromában (korai invasiv versus belgyógyászati kezelés)
20 17.3 Placebo 18 P=NS IV GP IIb/IIIa 16 14.3 14 12 10.5 10.1 Death or MI 10 8 6 Interaction P<.02 Boersma and colleagues conducted a meta-analysis of 6 randomized trials of GP IIb/IIIa inhibitors in patients with acute coronary syndrome (ACS) who were not routinely scheduled to undergo early coronary revascularization. The primary outcome measure was death or nonfatal myocardial infarction (MI) at 30 days. An analysis of cardiac endpoints showed that in patients undergoing percutaneous coronary intervention or coronary artery bypass graft within 5 days of randomization, the rate of death or MI within 30 days decreased significantly in those receiving GP IIb/IIIa inhibitors compared with patients receiving placebo (14.3% vs 17.3%; P=.0001). Death or MI rates were also reduced in patients taking GP IIb/IIIa inhibitors, whether they underwent early revascularization or not (10.1% vs 10.5%). 4 2 Intervention Medical Treatment (N=5847) (N=25,555) ACS, acute coronary syndrome; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; NS, not significant. Boersma E, et al. Lancet. 2002;359: References Boersma E, Harrington RA, Moliterno DJ, et al. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: a meta-analysis of all major randomized clinical trials. Lancet. 2002;359:
 who were not routinely scheduled to undergo early coronary revascularization. The primary outcome measure was death or nonfatal myocardial infarction (MI) at 30 days. An analysis of cardiac endpoints showed that in patients undergoing percutaneous coronary intervention or coronary artery bypass graft within 5 days of randomization, the rate of death or MI within 30 days decreased significantly in those receiving GP IIb/IIIa inhibitors compared with patients receiving placebo (14.3% vs 17.3%; P=.0001). Death or MI rates were also reduced in patients taking GP IIb/IIIa inhibitors, whether they underwent early revascularization or not (10.1% vs 10.5%) Intervention. Medical Treatment. (N=5847) (N=25,555) ACS, acute coronary syndrome; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; NS, not significant. Boersma E, et al. Lancet. 2002;359: References. Boersma E, Harrington RA, Moliterno DJ, et al. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: a meta-analysis of all major randomized clinical trials. Lancet. 2002;359:")
97
Gp IIb/IIIa bénítók hatása diabetesben
30 napos halálozás Trial N Odds Ratio & 95% Cl Placebo IIb/IIIa PURSUIT PRISM PRISM-PLUS GUSTO IV PARAGON A PARAGON B Pooled 2163 687 362 1677 412 1157 6458 P=.33 P=.07 P=.17 P=.022 P=.51 P=.93 P=.007 6.1% 4.2% 6.7% 7.8% 6.2% 4.8% 5.1% 1.8% 3.6% 5.0% 4.6% 4.9% Breslow-Day: P=.50 IIb/IIIa Better Placebo Better OR=0.74 Roffi M, et al. Circulation. 2001;104: (with permission)
")
98
Gp IIb/IIIa blokkolók PCI esetén
Csak magas rizikójú betegnek (ACS/AMI, bypass-graft, krónikus occlusio, látható intracoronariás thrombus) érdemes adni Eptifibatid kettős bolus (180 ug/kg i.v. 10 perc után ismét), majd fenntartó: 2 ug/tskg/min, vagy tirofiban (vagy abciximab) PCI előtt kezdve, mintegy órán át folytatva USD
 érdemes adni. Eptifibatid kettős bolus (180 ug/kg i.v. 10 perc után ismét), majd fenntartó: 2 ug/tskg/min, vagy tirofiban (vagy abciximab) PCI előtt kezdve, mintegy órán át folytatva USD.")
Hasonló előadás