Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Mesterséges táplálás Molnár Zsolt AITI

2
Alapfogalmak Mesterséges táplálás Energia szükséglet: Bevitel módja
25-30 kcal/kg/nap Szénhidrát: 50-70% Zsír: % Fehérje: 10-20% ( g/kg/nap aminosav) Vitaminok, nyomelemek Bevitel módja Enterális Parenterális 10 10
 Vitaminok, nyomelemek. Bevitel módja. Enterális. Parenterális")
3
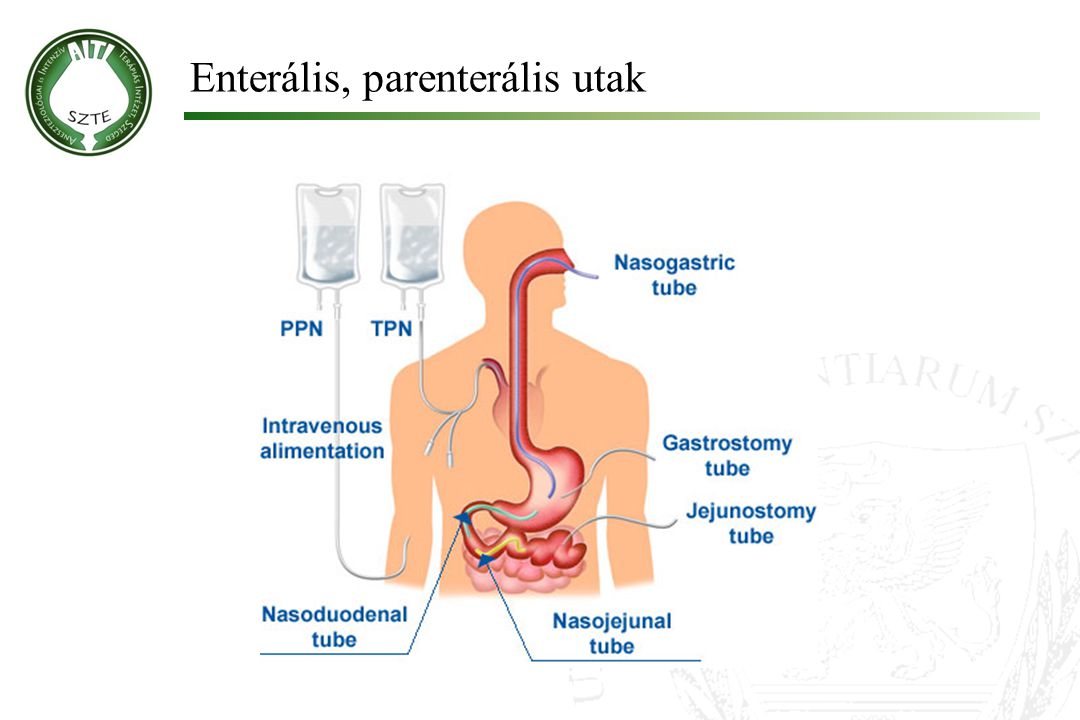
Enterális, parenterális utak
10 10
4
Betegmegelégedettség
„That tube went all the way to my stomach - and they put it in while I was conscious - nice! Made me feel better though ;-)” 10 10
")
5
Mi újat hozott az elmúlt 25 év a táplálásban?
Jobb technikai eszközök „All-in-one” készítmények Glutamin pótlás Koncepciózus vércukor kontroll Wernerman J. In: 25 Years of Progress and Innovation in Intensive Care Medicine 2007 10 10

6
Égést követő TOF, szepszis után 4 héttel…

7
Vád/önvád oka ≠

8
Bevezetés Táplálás filozófia 25 évvel ezelőtt Elméleti alapja
„Bigger is better” azaz „hyper-alimentáció” Wernerman J. In: 25 Years of Progress and Innovation in Intensive Care Medicine 2007 Elméleti alapja Nitrogén egyensúly Munro HN, et al. Biochemical aspects of protein metablism, New York and London. Academic Press 1963 Gyakorlati bizonyosságát Mért magas energiafogyasztás Wilmore DW. The Metabolic Management of the Critically Ill. New York and London: Plenum Medical Books 1977 10 10

9
„Alul-”, és „Túltáplálás”
Alultáplálás: Hosszabb ITO kezelés Hosszabb lélegeztetés Gyakoribb infekciós szövődmények Villet S, et al. Clin Nutr 2005; 24: 502-9 Rubinson L, et al. Crit Care Med 2004; 32: 350-7 Túltáplálás: Hosszabb ITO és kórházi ápolási idő Hányás, aspiráció, hasmenés Hyperlipidaemia, hyperglikémia Stapleton RD, et al. Proc AmThorac Soc 2006; 3: A737 10 10

10
PN indikációi Nem működő, vagy súlyosan károsodott emésztőrendszer
ASPEN Task Force. J Parenter Enteral Nutr 2002; 26: 1SA–138SA EN kontraindikált, vagy <40% energia igény/5 nap Etikailag elfogadható: várható túlélés ≥14 nap Nardo P, et al. Clin Nutr 2008; 27: Időzítés Minél előbb, EN + PN az első napokban Heidegger CP, et al. Curr Opin Crit Care. 2008; 14: 10 10

11
PN + adjuváns kezelés Immun-táplálás (glutamin)
Javítja a túlélést Goeters C, et al. Crit Care Med 2002; 30: Griffiths R, et al. Nutrition 1997; 13: Biztonságos Berg A, et al. In: Yearbook of ICEM 2009; pp: Víz-, és zsír-oldékony vitaminok: 1 amp/nap Nyomelemek: 1 amp/nap Nardo P, et al. Clin Nutr 2008; 27: 10 10

12
Mennyi legyen az optimális?
Kalóriaibevitel: amennyi kell Mennyi legyen az optimális?

13
Energiaigény becslése
Harris-Benedict formula Nem, kor, testsúly, testmagasság Kompenzációs faktor Long CL et al. JPEN 1979; 3: 452–6 Ireton-Jones Kor, testsúly, nem, + égés + trauma Ireton-Jones CS, et al. J Burn Care Rehabil 1992;13:330–3 Frankenfield Percventiláció, Hb, szepszis Frankenfield DC, et al. J Trauma 1994;18:398–403 Fusco Kor, magasság, testsúly Fusco MA, et al. JPEN 1995;19(suppl):18S 10 10
:18S")
14
Energiaigény mérése Indirekt kalorimetria Fick elv
O2 fogyasztás/ CO2 termelés „Arany standard” Feurer I, et al. Nutr Clin Pract 1986;1:43–9 Fick elv PA-katéter CO, Ca-vO2 Liggett SB, et al. Chest 1987;91:562–6 10 10

15
Energiaigény becslése – hátrányok, hibaforrások
Harris-Benedict, Ireton-Jones, Frankenfield, Fusco EI nő: Láz, hidegrázás Légzési munka Fájdalom, stressz, fizio, látogatás, stb Szepszis Katekolaminok EI csökken: Hypotermia Szedáció, altatás IPPV/CPAP MOF McClave SA, et al. Nut Pract 1992; 9: 61-8 Mint minden pontrendszer, ezek sem számolnak azzal, hogy tőbb, egyes paramétert befolyásoló tényező egyszerre történhet. Csak a beteg hiányzik a pontrendszerekből 10 10

16
Energiaigény mérése – hátrányok, hibaforrások
Indirekt kalorimetria Bonyolult, időigényes, drága Szigetelés, FiO2<60%, „steady state” percig(!) Adott „pillanatra” vonatkozik Browning JA, et al. Crit Care Med 1982; 10: 82–5 Hennenberg S, et al. Crit Care Med 1987; 15: 8–13 Fick elv P-A katéterezés SvO2<60%, „flow-dependent O2 supply” (ARDS,sepsis) „Mathematical coupling” Vincent JL, et al. Am Rev Respir Dis 1990; 142: 2–7 Tuchschmidt J, et al. Crit Care Med 1991; 19: 664–71 Mathematical coupling 10 10
 Adott „pillanatra vonatkozik. Browning JA, et al. Crit Care Med 1982; 10: 82–5. Hennenberg S, et al. Crit Care Med 1987; 15: 8–13. Fick elv. P-A katéterezés. SvO2<60%, „flow-dependent O2 supply (ARDS,sepsis) „Mathematical coupling Vincent JL, et al. Am Rev Respir Dis 1990; 142: 2–7. Tuchschmidt J, et al. Crit Care Med 1991; 19: 664–71. Mathematical coupling")
17
Caloric Intake in Medical ICU Patients: consistency of care with guidelines and relationship to clinical outcomes. Krishnan JA, et al. Chest 2003; 124: 9-18 kcal/kg/nap The cumulative average caloric intake since ICU admission for each of 187 participants () is shown. For example, a participant’s cumulative average caloric intake for ICU day 5 is the mean for days 1 to 5. Similarly, a participant’s cumulative average caloric intake for ICU day 10 is the mean caloric intake for ICU days 1 to 10. The last cumulative average caloric intake for each participant thus represents the average caloric intake from nutritional support over all ICU days for that participant. The mean caloric intake for each ICU day (x) for all participants in the ICU is also shown. The horizontal line at caloric intake represents 100% of the target caloric intake recommended by ACCP guidelines 10 10
 is shown. For example, a participant’s cumulative average caloric intake for ICU day 5 is the mean for days 1 to 5. Similarly, a participant’s cumulative average caloric intake for ICU day 10 is the mean caloric intake for ICU days 1 to 10. The last cumulative average caloric intake for each participant thus represents the average caloric intake from nutritional support over all ICU days for that participant. The mean caloric intake for each ICU day (x) for all participants in the ICU is also shown. The horizontal line at caloric intake represents 100% of the target caloric intake recommended by ACCP guidelines")
18
Szignifikánsan jobb OR:
Caloric Intake in Medical ICU Patients: consistency of care with guidelines and relationship to clinical outcomes. Krishnan JA, et al. Chest 2003; 124: 33-66% (II) vs >66% (III) Szignifikánsan jobb OR: Kórházi túlélés Spontán légzés – kiadáskor Szepszis mentes – kiadáskor 25% > Szignifikánsan több: Nozokomiális infekció Rubinson L et al. CCM 2004; 32: 350 ORs and 95% CIs for hospital discharge alive in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = Middle, B: ORs and 95% CIs for spontaneous ventilation prior to ICU discharge in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = Bottom, C: ORs and 95% CIs for ICU discharge without sepsis in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = An OR of > 1.0 indicates a greater likelihood of outcome compared to tertile I. An OR of < 1.0 indicates a lower likelihood of outcome compared to tertile I. * = adjusted for SAPS II score, serum albumin level, body mass index, gastric residuals, and route of feeding in a multivariable logistic regression model 10 10
 vs >66% (III) Szignifikánsan jobb OR: Kórházi túlélés. Spontán légzés – kiadáskor. Szepszis mentes – kiadáskor. 25% > Szignifikánsan több: Nozokomiális infekció. Rubinson L et al. CCM 2004; 32: 350. ORs and 95% CIs for hospital discharge alive in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = Middle, B: ORs and 95% CIs for spontaneous ventilation prior to ICU discharge in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = Bottom, C: ORs and 95% CIs for ICU discharge without sepsis in patients with tertiles II and III of caloric intake. Hosmer-Lemeshow test statistic for multivariable model, p = An OR of > 1.0 indicates a greater likelihood of outcome compared to tertile I. An OR of < 1.0 indicates a lower likelihood of outcome compared to tertile I. * = adjusted for SAPS II score, serum albumin level, body mass index, gastric residuals, and route of feeding in a multivariable logistic regression model")
19
Szepszis, immobilizáció

20
Mitochondrial function in sepsis: Respiratory versus leg muscle
Fredriksson K, et al. Crit Care Med 2007; 35: S449-S453 The energy produced in the mitochondrion comes from the oxidation of several metabolites, such as glucose and fat. These are broken down in the cell to, respectively, pyruvate and free fatty acids. The mitochondrion takes up pyruvate and free fatty acids from the cytosol of the cell. Within the mitochondrial matrix, these metabolites are transformed into acetyl coenzyme A and go through the citric acid cycle (Fig. 1). In this cycle, two reducing factors, nicotinamide adenine dinucleotide and flavin adenine dinucleotide, are produced, along with some adenosine 5'-triphosphate (ATP). However, the major part of the ATP produced in the mitochondrion is produced in the respiratory chain, or electron transport chain. The respiratory chain consists of five enzyme complexes that transport the donated electrons between each other. Electrons are donated from the nicotinamide adenine dinucleotide and flavin adenine dinucleotide produced in the citric acid cycle to complexes 1 and 2, the first and second complex of the chain
. In this cycle, two reducing factors, nicotinamide adenine dinucleotide and flavin adenine dinucleotide, are produced, along with some adenosine 5 -triphosphate (ATP). However, the major part of the ATP produced in the mitochondrion is produced in the respiratory chain, or electron transport chain. The respiratory chain consists of five enzyme complexes that transport the donated electrons between each other. Electrons are donated from the nicotinamide adenine dinucleotide and flavin adenine dinucleotide produced in the citric acid cycle to complexes 1 and 2, the first and second complex of the chain.")
21
Mitochondrial function in sepsis: Respiratory versus leg muscle
Fredriksson K, et al. Crit Care Med 2007; 35: S449-S453 Fekete: sepsis+MOF Szürke: kontroll (elektív sebészeti betegek) Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate
 Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate.")
22
Atrophy and Impaired Muscle Protein Synthesis during Prolonged Inactivity and Stress
Paddon-Jones D, et al. J Clin Endocrinol Metab Dec;91(12): Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate
: Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate.")
23
Atrophy and Impaired Muscle Protein Synthesis during Prolonged Inactivity and Stress
Paddon-Jones D, et al. J Clin Endocrinol Metab Dec;91(12): Variable Value Age (yr) 27 ± 1 Height (cm) 180 ± 3 Body mass (prebed rest) (kg) 82.8 ± 4.0 Body mass change (kg) –2.8 ± 0.6 Upper body lean mass change (g) –679.8 ± Lean leg mass change (g)2 – ± Body fat mass change (g) –95.6 ± 288.1 1RM leg ext strength change (%) –28.4 ± 4.41 Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate 1 Significant pre- to postbed rest change (P < 0.05). 2 Loss of lean muscle mass (dual-energy x-ray absorptiometry) from both legs.
: Variable. Value. Age (yr) 27 ± 1. Height (cm) 180 ± 3. Body mass (prebed rest) (kg) 82.8 ± 4.0. Body mass change (kg) –2.8 ± 0.6. Upper body lean mass change (g) –679.8 ± Lean leg mass change (g)2. – ± Body fat mass change (g) –95.6 ± RM leg ext strength change (%) –28.4 ± Activities (mean ± sd) of citrate synthase (top), complex 1 (middle), and complex 4 (bottom) in respiratory (serratus anterior) and locomotive (vastus lateralis) muscle of patients with sepsis-induced multiple organ failure (black) and age-matched control patients undergoing elective surgery (gray). The decreased mitochondrial content in leg skeletal muscle is accompanied by a decrease in the concentrations of energy-rich phosphates and an increased concentration of lactate. 1 Significant pre- to postbed rest change (P < 0.05). 2 Loss of lean muscle mass (dual-energy x-ray absorptiometry) from both legs.")
24
Ahogyan csináltam 2009-ig…
Szupportív terápia „Best standard care” DO2/VO2 rendezése Rendszeres vérgáz (artériás, centrális vénás) Szoros vércukor kontroll 6-8 mmol/l Korai, kontrollált enterális táplálás 30 ml/ó: gyomoraspiráció 3-4 órával kezdés után 50-60 ml/ó ~ 1500 kcal/nap Korai tracheostomia Ébresztés, aktív mozgás Kommunikáció a beteggel „Agresszív” leszoktatás Passzív mozgatás: kontraktúráktól véd Izomerő: aktív torna 10 10
 Szoros vércukor kontroll 6-8 mmol/l. Korai, kontrollált enterális táplálás. 30 ml/ó: gyomoraspiráció 3-4 órával kezdés után ml/ó ~ 1500 kcal/nap. Korai tracheostomia. Ébresztés, aktív mozgás. Kommunikáció a beteggel. „Agresszív leszoktatás. Passzív mozgatás: kontraktúráktól véd. Izomerő: aktív torna")
25
…és ahogyan fogom Ugyanúgy, de…
Korai, kontrollált E, esetleg P táplálás 30 ml/ó: gyomoraspiráció 3-4 órával kezdés után 50-60 ml/ó ~ 1500 kcal/nap Vércukor kontroll 8-10 mmol/l a célérték (6-8 mmol/l helyett) Finfer S, et al. N Engl J Med 2009; 360: Minden TPN-t kapó beteg kap: Nyomelem + vitamin (1a/nap) Glutamin 10 10
 Finfer S, et al. N Engl J Med 2009; 360: Minden TPN-t kapó beteg kap: Nyomelem + vitamin (1a/nap) Glutamin")
26
Összefoglalás Krónikus éhezés ≠ kritikus állapot izomvesztésével
Máshogy kezelünk ma, mint 25 évvel ezelőtt Kevésbé megterhelő a betegnek A kevesebb sokszor több A számított kalória 25-60%-át adjuk - nem ártunk, sőt! PRCT-re lenne szükség… Az aktív mozgást nem pótolja semmi 10 10

27
A betegnek mindig igaza van:
Mottó A betegnek mindig igaza van: ha nem éhes, nem etetem. 10 10

Hasonló előadás














 Mikortól? (minél előbb)>")




