Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
EKG a klinikumban dr. Szilágyi Szabolcs Semmelweis Egyetem
Kardiológiai Tanszék

2
QT szakasz Q elejétől T végéig Szívfrekvencia befolyásolja
QTc: QT / √ RR, (RR s –ban) QTc> 440 ms kóros QT-t nyújtja: BKH, IV vezetési zavar, AMI, ACS, akut PE, myocarditis, hypoCa+ Mg, gyógyszerek ( amiodarone, prokainamid, kinidin) QT-t rövidíti: digitalis, hyperCa, hyperthyreosis
 QTc> 440 ms kóros. QT-t nyújtja: BKH, IV vezetési zavar, AMI, ACS, akut PE, myocarditis, hypoCa+ Mg, gyógyszerek ( amiodarone, prokainamid, kinidin) QT-t rövidíti: digitalis, hyperCa, hyperthyreosis.")
3
U hullám T után időnként látható kis hullám
Jelentősége pontosan nem ismert Polaritása a t-vel egyezik Legnagyobb amplitúdó V3-ban Amplitúdó nő: hypoK, BKH, bradycardia, atléta, digitalis, kinidin Negatív U hullám mindig kóros, ISZB, BKH, ha terhelésre: rossz kamrafunkció

4
Hyperkalaemia Magas csúcsos, szimmetrikus T hullámok
PR szakasz és a QRS progresszív megnyúlása P hullám eltűnik (pitvari csend) QRS sinus hullám-szerű, akár extrém kiszélesedése Végállapot: kamrai csend, vagy VF Társulhat: vezetési zavar (JTSZB, BTSZB, BAH, bifascicularis blokk, AV blokk) Az EKG kép és a hyperkalaemia mértéke nem korrelál!
 QRS sinus hullám-szerű, akár extrém kiszélesedése. Végállapot: kamrai csend, vagy VF. Társulhat: vezetési zavar (JTSZB, BTSZB, BAH, bifascicularis blokk, AV blokk) Az EKG kép és a hyperkalaemia mértéke nem korrelál!")
5
Hyperkalaemia Gyakori: veseelégtelenség, DM
Fontos az EKG monitorozása - progresszió Az EKG kép alakulását befolyásolhatja: a kialakulás üteme, Na, Ca-szint egyéb társbetegségek (pl kamrahypertrophia) 7 mmol/l felett potenciálisan életveszélyes EKG eltérések észlelése esetén a terápiát haladéktalanul meg kell kezdeni! Hatásmechanizmus: magas EC K koncentráció csökkenti a nyugalmi membránpotenciált – parciálisan depolarizálja – az ingerelhetőség nő Később: a peristens depolarizáció inaktiválja a Na csatornákat – csökken az ingerelhetőség – vezetési zavarok
 7 mmol/l felett potenciálisan életveszélyes. EKG eltérések észlelése esetén a terápiát haladéktalanul meg kell kezdeni! Hatásmechanizmus: magas EC K koncentráció csökkenti a nyugalmi membránpotenciált – parciálisan depolarizálja – az ingerelhetőség nő. Később: a peristens depolarizáció inaktiválja a Na csatornákat – csökken az ingerelhetőség – vezetési zavarok.")
6
Hypokalaemia Az EKG eltérések nem korrelálnak a K szinttel!
T hullám amplitúdója csökken, az U hullámé nő – egybeolvadva „hosszú QT” T/U ≤ 1 - II, V3 ST depresszió >0,5 mm - V1-3 Egyéb eltérések: Magasabb és szélesebb P hullámok QRS szélessége nőhet kifejezettebb ST depresszió, T hullám inverzió

7
Hypercalcaemia QT intervallum csökken (rövidebb ST szakasz)
T hullám proximalis része rövidebb Egyéb, időnként megfigyelhető eltérések: PR megnyúlás QRS amplitúdó növekedése Bifázisos T Típusos: hyperparathyreosis malignus betegségek

8
Hypocalcaemia QT szakasz megnyúlása – EAD, triggerelt mechanizmusú aritmiák Hosszabb lesz az ST szakasz (a membrán repolarizáció megkezdődése késik) T hullám nem változik jelentősen Jellegzetes: hypoparathyreosis D vitamin hiány vagy rezisztencia hypomagnesaemia (malabsorptio, alkoholizmus) akut pancreatitis sepsis, súlyos betegség osteoblastos metastasis ( mell és prostatacc)
 T hullám nem változik jelentősen. Jellegzetes: hypoparathyreosis. D vitamin hiány vagy rezisztencia hypomagnesaemia (malabsorptio, alkoholizmus) akut pancreatitis. sepsis, súlyos betegség. osteoblastos metastasis ( mell és prostatacc)")
9
Hypomagnesaemia Megnyúlt PQ SA és vagy AV blokk QRS kiszélesedése
QT nem változik Önmagában ritka, legtöbbször hypokalaemiával együtt

10
Hypothermia 34 C alatti hőmérséklet Az ingervezetés diffúz lelassulása
(nő RR, PR, QRS, QT) Jellegzetes ún. Osborne hullám a QRS-t követően a mellkasi elvezetésekben (mértéke korrelál a hypothermia fokával)
 Jellegzetes ún. Osborne hullám a QRS-t követően a mellkasi elvezetésekben. (mértéke korrelál a. hypothermia fokával)")
11
Digitalis Centrálisan szimpatikus aktivitásfokozódás – fokozódik az automácia és az ingerelhetőség Nő a perifériás vagus tónus – a normál ingerképző és ingervezető rendszer gátlása Jellegzetes ST depresszió Jellegzetes: VES Pitvari tachy+ AV blokk Akcelerált junkcionális ritmus

12
Triciklikus antidepresszáns túladagolás
Hatás: gyors NA-csatornák blokádja QRS kiszélesedik (160 ms felett 50 %-ban kamrai ritmuszavarok!) His-Purkinje ill. interventricularis vezetési zavar (különösen JTSZB) PR és QT intervallum megnyúlása Sinus tachycardia – vagolyticus hatás miatt
 His-Purkinje ill. interventricularis vezetési zavar. (különösen JTSZB) PR és QT intervallum megnyúlása. Sinus tachycardia – vagolyticus hatás miatt.")
14
Tüdőembólia Nem EKG diagnózis, de diagnosztikus segítség lehet
Nagy PE – mindig van sinus tachycardia Egyéb lehetséges eltérések: SIQ3, átmeneti zóna jobbra tolódása mellkasi elvezetésekben negatív T jobb kamrai vezetési zavar ( inkomplett) JTSZB P pulmonale
 JTSZB. P pulmonale.")
17
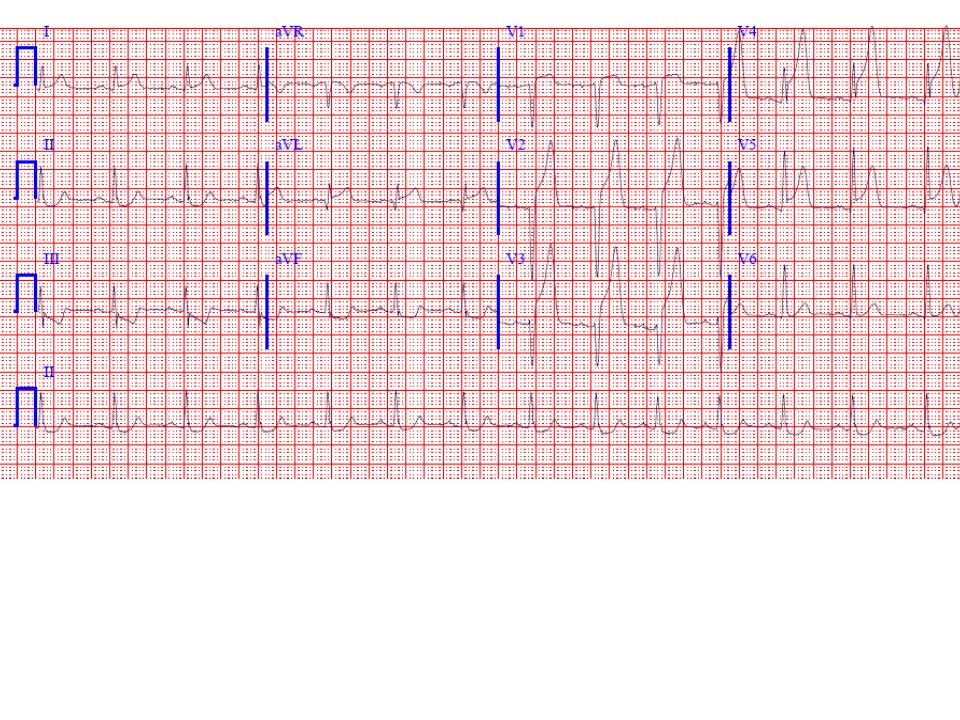
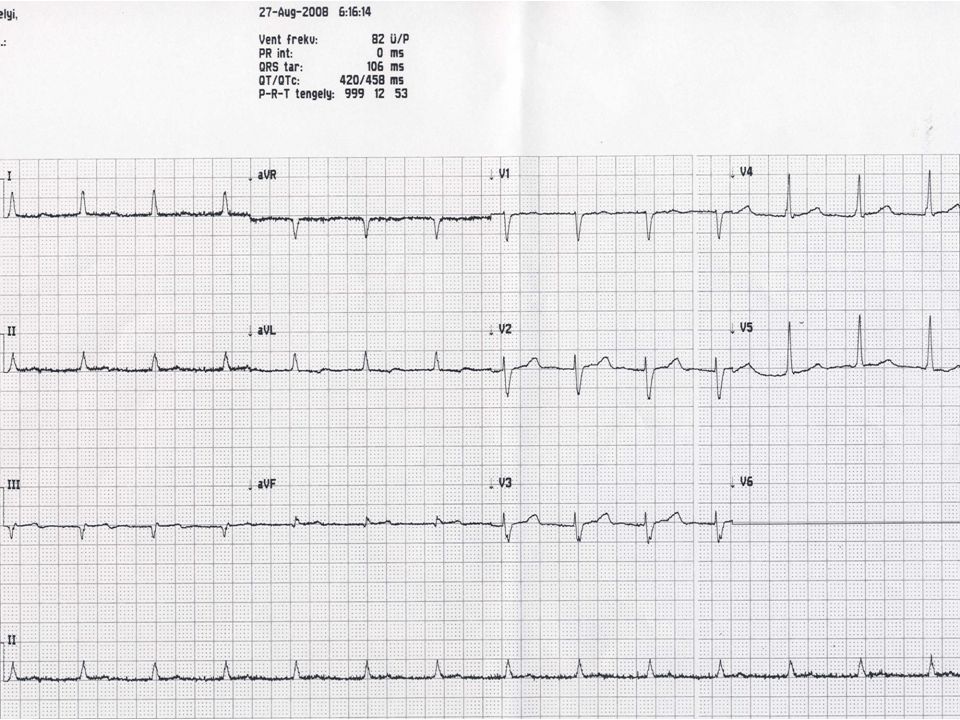
ECG shows sinus rhythm with left ventricular hypertrophy (LVH), left atrial abnormality and tall peaked T waves best seen in the precordial leads (with non-specific infero-lateral ST depressions). Also present are left axis deviation consistent with left anterior fascicular block and a borderline long QT. Putting it all together, the peaked T waves indicate increased K+ (6.3 mEq/L) with LVH suggesting renal failure associated with hypertension, which was the case here. The long QT with stretchout ST segment phase goes with decreased calcium seen with renal failure as well. ST depressions could be from LVH or primary ischemia, in addition to multiple other causes. So when you see the triad of "tented" T waves (hyperkalemia) with long QT (ST segment prolongation consistent with hypocalcemia) and LVH (hypertension) the patient virtually always has renal failure.
 with LVH suggesting renal failure associated with hypertension, which was the case here. The long QT with stretchout ST segment phase goes with decreased calcium seen with renal failure as well. ST depressions could be from LVH or primary ischemia, in addition to multiple other causes. So when you see the triad of tented T waves (hyperkalemia) with long QT (ST segment prolongation consistent with hypocalcemia) and LVH (hypertension) the patient virtually always has renal failure..")
18
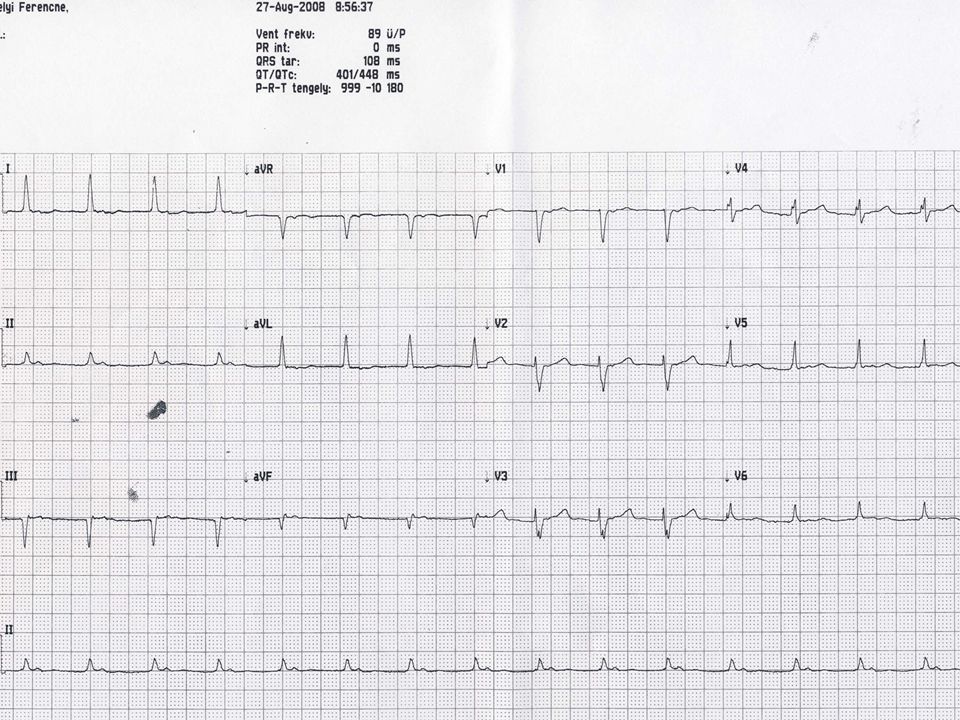
What's up here. Difficulty ratingAnswer:Serum K+. It was 7. 7 mEq/L
What's up here? * * Difficulty ratingAnswer:Serum K+. It was 7.7 mEq/L. Note the relatively tall peaked (tented) T waves that are a classic sign of mild-moderate hyperkalemia. With more severe elevations, the QRS will widen, as will the PR, and the P wave amplitude will diminish, resulting in a junctional or idioventricular-type rhythm eventually.
 T waves that are a classic sign of mild-moderate hyperkalemia. With more severe elevations, the QRS will widen, as will the PR, and the P wave amplitude will diminish, resulting in a junctional or idioventricular-type rhythm eventually.")
19
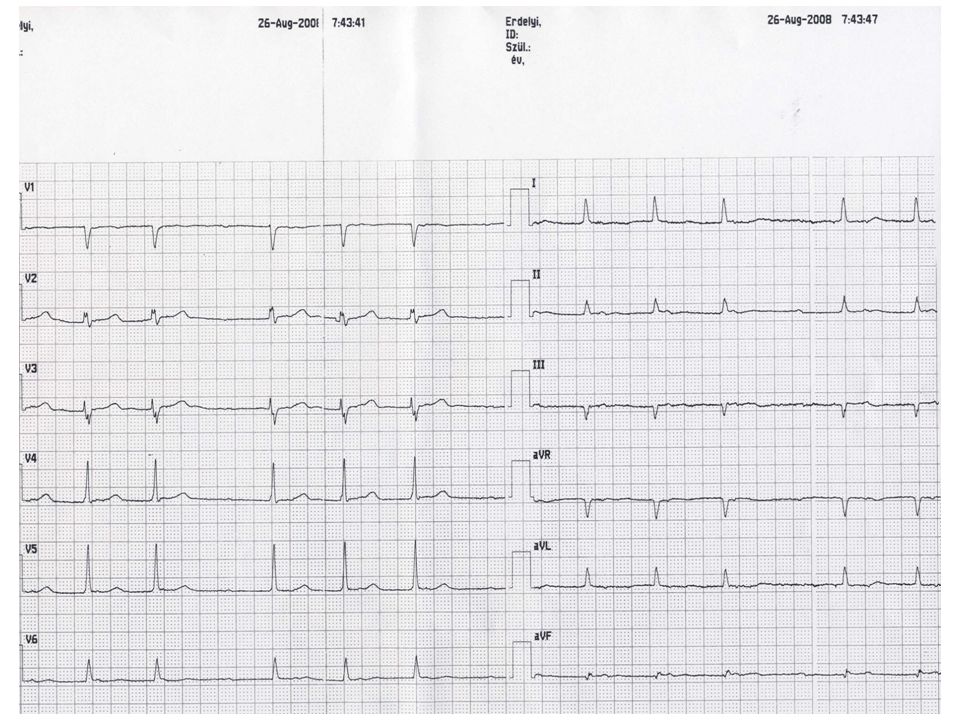
Hyperkalemia (K+ = 8. 7 mEq/L) secondary to acute renal failure
Hyperkalemia (K+ = 8.7 mEq/L) secondary to acute renal failure. The ECG shows symmetrically peaked ("tented") T waves associated with potassium levels in excess of 6 mEq/L. The tracing also shows broad and flattened sinus P waves that may precede frank sino-ventricular conduction seen with severe hyperkalemia (i.e., conduction from the sinus node to the ventricles through specialized inter-nodal tissue without atrial depolarization). This conduction pattern may simulate a junctional rhythm. The narrow QRS complex in this tracing is somewhat atypical for severe hyperkalemia. Milder degrees of hyperkalemia may actually facilitate AV conduction. Note that T wave peaking with hyperkalemia is a relative finding: the absolute magnitude of the T waves cannot be used to rule in or rule out hyperkalemia. Indeed, in some cases of hyperkalemia with left ventricular hypertrophy, the T wave peaking may affect inverted T waves or cause relative normalization. The presence of relatively low voltage and sinus bradycardia in this clinical setting should also raise consideration of hypothyroidism/myxedema, which by itself usually also causes T wave flattening.
 secondary to acute renal failure. The ECG shows symmetrically peaked ( tented ) T waves associated with potassium levels in excess of 6 mEq/L. The tracing also shows broad and flattened sinus P waves that may precede frank sino-ventricular conduction seen with severe hyperkalemia (i.e., conduction from the sinus node to the ventricles through specialized inter-nodal tissue without atrial depolarization). This conduction pattern may simulate a junctional rhythm. The narrow QRS complex in this tracing is somewhat atypical for severe hyperkalemia. Milder degrees of hyperkalemia may actually facilitate AV conduction. Note that T wave peaking with hyperkalemia is a relative finding: the absolute magnitude of the T waves cannot be used to rule in or rule out hyperkalemia. Indeed, in some cases of hyperkalemia with left ventricular hypertrophy, the T wave peaking may affect inverted T waves or cause relative normalization. The presence of relatively low voltage and sinus bradycardia in this clinical setting should also raise consideration of hypothyroidism/myxedema, which by itself usually also causes T wave flattening.")
20
Pericarditis

21
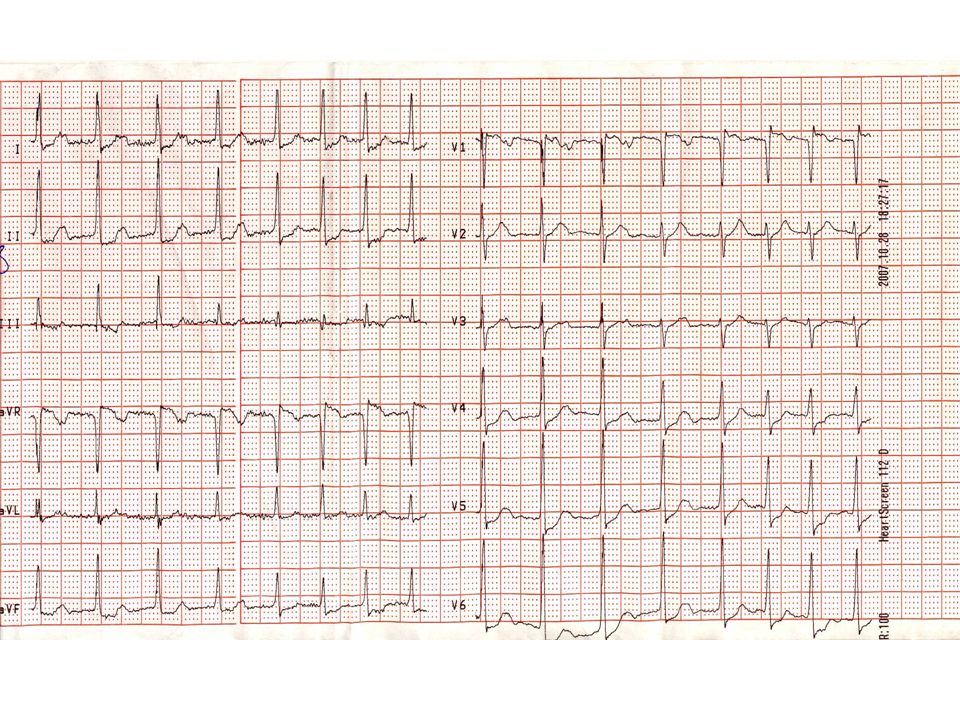
A 65-year-old man. What should you do before calling cardiology fellow for what be called a "hyperacute myocardial infarction" pattern in this case? * * Difficulty ratingAnswer:Put the "lytes" on! This is classic hyperkalemia with tall peaked T waves, along with PR prolongation and underlying left ventricular hypertrophy (LVH) (patient has renal disease with hypertension). Note QRS prolongation also seen with moderate-severe hyperkalemia. Potassium here was 9.6mEq/L. Not all tall positive T waves are "hyperacute." The latter term should be reserved for increased T wave positivity secondary to transmural ischemia. Major clues include narrowness (tenting) of T waves along with other findings noted above
 (patient has renal disease with hypertension). Note QRS prolongation also seen with moderate-severe hyperkalemia. Potassium here was 9.6mEq/L. Not all tall positive T waves are hyperacute. The latter term should be reserved for increased T wave positivity secondary to transmural ischemia. Major clues include narrowness (tenting) of T waves along with other findings noted above.")
22
Dx: Hyperkalemia (7. 6 mEq/L) secondary to renal failure
Dx: Hyperkalemia (7.6 mEq/L) secondary to renal failure. The ECG demonstrates findings consistent with severe hyperkalemia -- most importantly marked widening of the QRS complex. The QRS complex here shows a left bundle branch block (LBBB) morphology with left axis deviation. However, the QRS duration (about 240 ms) is much wider than seen with an "uncomplicated" LBBB or just with left anterior fascicular block due to intrinsic conduction disease. There is also peaking of the T waves with prolongation of the PR interval and flattening of the P waves. If the hyperkalemia is left untreated, the ECG will progress to a sinusoidal pattern and eventually asystole with subsequent hemodynamic collapse and death.
 secondary to renal failure. The ECG demonstrates findings consistent with severe hyperkalemia -- most importantly marked widening of the QRS complex. The QRS complex here shows a left bundle branch block (LBBB) morphology with left axis deviation. However, the QRS duration (about 240 ms) is much wider than seen with an uncomplicated LBBB or just with left anterior fascicular block due to intrinsic conduction disease. There is also peaking of the T waves with prolongation of the PR interval and flattening of the P waves. If the hyperkalemia is left untreated, the ECG will progress to a sinusoidal pattern and eventually asystole with subsequent hemodynamic collapse and death.")
23
b) The ECG findings are diagnostic of severe hyperkalemia
b) The ECG findings are diagnostic of severe hyperkalemia. The two key features are a very wide QRS complex (intraventricular conduction delay) and no evident P waves so that the underlying atrial mechanism cannot be determined. (The bizarre QRS morphology seen here with wide terminal R waves in V1 and V2 and very wide S waves in other leads is also not uncommon in this context; although a variety of other wide complex morphologies are also seen with severe hyperkalemia. See other Wave-Maven cases for multiple other examples.) Of further note, ST elevations localized in leads V1-V2, as seen here, are also sometimes observed with severe hyperkalemia in the absence of acute ischemia/myocardial infarction (MI), although the latter cannot be excluded by the ECG alone. CK-MB and troponin assays were negative in this case. The patient had severe hyperkalemia with combined renal and hepatic failure (hepato-renal syndrome).
 The ECG findings are diagnostic of severe hyperkalemia. The two key features are a very wide QRS complex (intraventricular conduction delay) and no evident P waves so that the underlying atrial mechanism cannot be determined. (The bizarre QRS morphology seen here with wide terminal R waves in V1 and V2 and very wide S waves in other leads is also not uncommon in this context; although a variety of other wide complex morphologies are also seen with severe hyperkalemia. See other Wave-Maven cases for multiple other examples.) Of further note, ST elevations localized in leads V1-V2, as seen here, are also sometimes observed with severe hyperkalemia in the absence of acute ischemia/myocardial infarction (MI), although the latter cannot be excluded by the ECG alone. CK-MB and troponin assays were negative in this case. The patient had severe hyperkalemia with combined renal and hepatic failure (hepato-renal syndrome).")
24
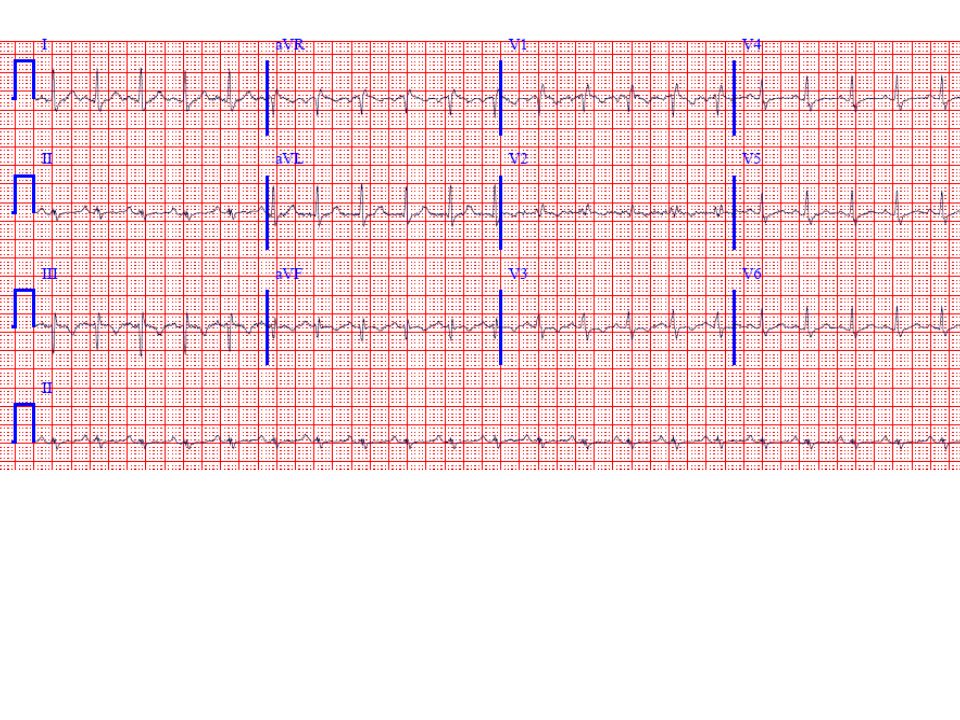
The ECG shows sinus rhythm with the following abnormalities a very short ST segment with a consequently short QT interval (about 300 msec here). The differential diagnosis of a short QT (lower limits are not well-defined) is much narrower than that of prolonged QT. The two chief causes of a short QT are hypercalcemia and digoxin therapy (associated with characteristic "scooping" of the ST-T complex). A third and relatively rare cause is hereditary short QT ("channelopathy"-related) that may be associated with ventricular arrhythmia and sudden cardiac arrest. Cardiac arrhythmias, however, are unusual with hypercalcemia; but AV block, sinus arrest, sino-atrial block, ventricular tachycardia, and cardiac arrest have been reported, usually in patients receiving rapid IV injections of calcium. This patient's serum calcium was 16 mg/dl. He was found to have hyperparathyroidism; at surgery, he had successful resection of a parathyroid carcinoma, an ususual cause of hypercalcemia.
 is much narrower than that of prolonged QT. The two chief causes of a short QT are hypercalcemia and digoxin therapy (associated with characteristic scooping of the ST-T complex). A third and relatively rare cause is hereditary short QT ( channelopathy -related) that may be associated with ventricular arrhythmia and sudden cardiac arrest. Cardiac arrhythmias, however, are unusual with hypercalcemia; but AV block, sinus arrest, sino-atrial block, ventricular tachycardia, and cardiac arrest have been reported, usually in patients receiving rapid IV injections of calcium. This patient s serum calcium was 16 mg/dl. He was found to have hyperparathyroidism; at surgery, he had successful resection of a parathyroid carcinoma, an ususual cause of hypercalcemia..")
25
Herediter rövid QT – SCD! Hyperparathyreosis
The ECG shows sinus rhythm with the following abnormalities a very short ST segment with a consequently short QT interval (about 300 msec here). The differential diagnosis of a short QT (lower limits are not well-defined) is much narrower than that of prolonged QT. The two chief causes of a short QT are hypercalcemia and digoxin therapy (associated with characteristic "scooping" of the ST-T complex). A third and relatively rare cause is hereditary short QT ("channelopathy"-related) that may be associated with ventricular arrhythmia and sudden cardiac arrest. Cardiac arrhythmias, however, are unusual with hypercalcemia; but AV block, sinus arrest, sino-atrial block, ventricular tachycardia, and cardiac arrest have been reported, usually in patients receiving rapid IV injections of calcium. This patient's serum calcium was 16 mg/dl. He was found to have hyperparathyroidism; at surgery, he had successful resection of a parathyroid carcinoma, an ususual cause of hypercalcemia. Hypercalcaemia Digitalis Herediter rövid QT – SCD! Hyperparathyreosis
. The differential diagnosis of a short QT (lower limits are not well-defined) is much narrower than that of prolonged QT. The two chief causes of a short QT are hypercalcemia and digoxin therapy (associated with characteristic scooping of the ST-T complex). A third and relatively rare cause is hereditary short QT ( channelopathy -related) that may be associated with ventricular arrhythmia and sudden cardiac arrest. Cardiac arrhythmias, however, are unusual with hypercalcemia; but AV block, sinus arrest, sino-atrial block, ventricular tachycardia, and cardiac arrest have been reported, usually in patients receiving rapid IV injections of calcium. This patient s serum calcium was 16 mg/dl. He was found to have hyperparathyroidism; at surgery, he had successful resection of a parathyroid carcinoma, an ususual cause of hypercalcemia. Hypercalcaemia. Digitalis. Herediter rövid QT – SCD! Hyperparathyreosis.")
26
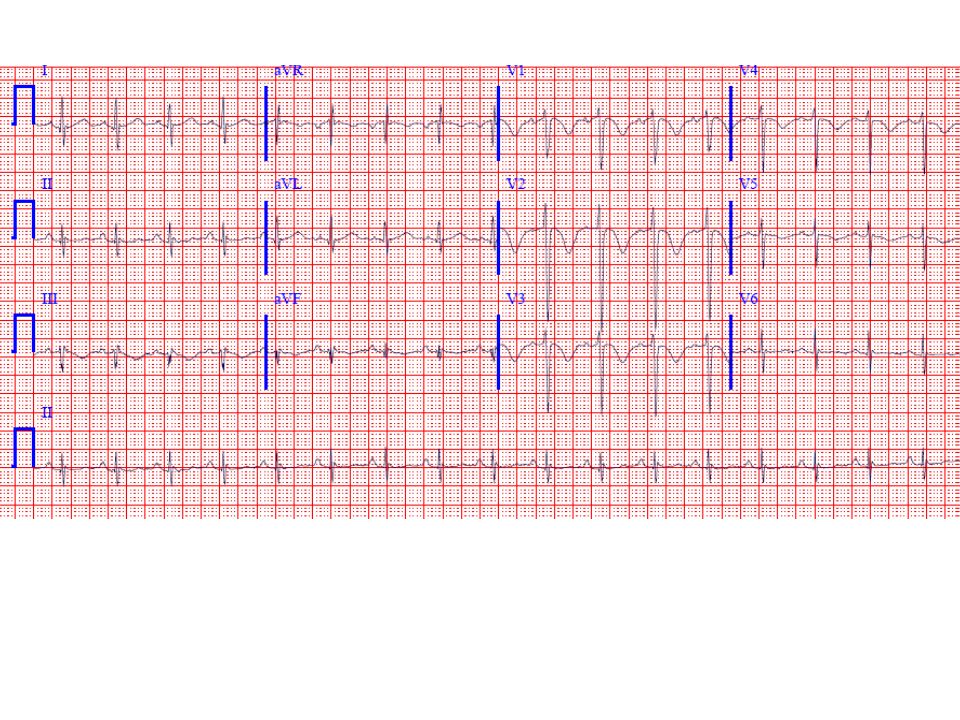
The ECG shows sinus bradycardia with diffuse T wave flattening or inversions, and markedly prominent U waves. These are best seen in leads V2 and V3, but are essentially invisible in lead aVL. The two most common causes of this finding are 1) Hypokalemia (K+ here was 2.4 mEq/L) and 2) Drugs, especially the class 1A antiarrhythmics (like quinidine, procainamide, disopyramide) and related agents (like the phenothiazines and tricyclics), etc. Patients with hereditary (congital) long QT syndromes due to "channelopathies" may show a similar finding (see Case 1). This ventricular repolarization prolongation pattern is of great importance because it identifies patients at high risk of torsade de pointes type of polymorphic ventricular tachycardia.
 Hypokalemia (K+ here was 2.4 mEq/L) and 2) Drugs, especially the class 1A antiarrhythmics (like quinidine, procainamide, disopyramide) and related agents (like the phenothiazines and tricyclics), etc. Patients with hereditary (congital) long QT syndromes due to channelopathies may show a similar finding (see Case 1). This ventricular repolarization prolongation pattern is of great importance because it identifies patients at high risk of torsade de pointes type of polymorphic ventricular tachycardia..")
27
Gyógyszerek ( Ia, III, antidepresszánsok) Congenitalis hosszú QT
The ECG shows sinus bradycardia with diffuse T wave flattening or inversions, and markedly prominent U waves. These are best seen in leads V2 and V3, but are essentially invisible in lead aVL. The two most common causes of this finding are 1) Hypokalemia (K+ here was 2.4 mEq/L) and 2) Drugs, especially the class 1A antiarrhythmics (like quinidine, procainamide, disopyramide) and related agents (like the phenothiazines and tricyclics), etc. Patients with hereditary (congital) long QT syndromes due to "channelopathies" may show a similar finding (see Case 1). This ventricular repolarization prolongation pattern is of great importance because it identifies patients at high risk of torsade de pointes type of polymorphic ventricular tachycardia. Hypokalaemia Gyógyszerek ( Ia, III, antidepresszánsok) Congenitalis hosszú QT TdP
 Hypokalemia (K+ here was 2.4 mEq/L) and 2) Drugs, especially the class 1A antiarrhythmics (like quinidine, procainamide, disopyramide) and related agents (like the phenothiazines and tricyclics), etc. Patients with hereditary (congital) long QT syndromes due to channelopathies may show a similar finding (see Case 1). This ventricular repolarization prolongation pattern is of great importance because it identifies patients at high risk of torsade de pointes type of polymorphic ventricular tachycardia. Hypokalaemia. Gyógyszerek ( Ia, III, antidepresszánsok) Congenitalis hosszú QT. TdP.")
28
30-yr-old man, not on medication. What waveform is prominent
30-yr-old man, not on medication. What waveform is prominent? What is the likely diagnosis, assuming prior normal ECG? * * Difficulty ratingAnswer:There are very (!) prominent U waves with Q-T(U) prolongation. He had severe hypokalemia (1.5 mEq/L) due to diarrhea. Calcium was normal, as was magnesium (remember pure hypocalcemia prolongs the ST segment primarily but does not give large U waves.) Obviously, this acquired-type long-QT(U) syndrome puts the subject at risk for torsade de pointes which he fortunately did not have before coming to hospital. The same type ECG may occur with drug-related QT(U) prolongation syndromes and with hereditary long QT(U) syndromes related to "channelopathies," including the Romano-Ward and Jervell Lange-Nielsen syndromes
 prominent U waves with Q-T(U) prolongation. He had severe hypokalemia (1.5 mEq/L) due to diarrhea. Calcium was normal, as was magnesium (remember pure hypocalcemia prolongs the ST segment primarily but does not give large U waves.) Obviously, this acquired-type long-QT(U) syndrome puts the subject at risk for torsade de pointes which he fortunately did not have before coming to hospital. The same type ECG may occur with drug-related QT(U) prolongation syndromes and with hereditary long QT(U) syndromes related to channelopathies, including the Romano-Ward and Jervell Lange-Nielsen syndromes.")
29
Minimalist/optimal medicine quiz
Minimalist/optimal medicine quiz. If you could do only one lab test, what would it be in this case? * * * Difficulty ratingAnswer:Check the calcium (and yes, of course albumin). It was low here at 8.2 mg/dl with minimally low albumin in patient post thyroidectomy. ECG shows QT prolongation. Most important is that QT is long in this case because the ST segment is stretched out. This relates to prolongation of the plateau phase of action potential which is prolonged with hypocalcemia. Ventricular repolarization can also be long because of 1) wide QRS; 2) flat, wide T waves (e.g. quinidine, sotalol, hypokalemia, etc); and/or 3) prominent U waves melding with T wave. The latter two syndromes, representing dispersion of ventricular refractoriness, are most likely to be associated with torsade de pointes.
. It was low here at 8.2 mg/dl with minimally low albumin in patient post thyroidectomy. ECG shows QT prolongation. Most important is that QT is long in this case because the ST segment is stretched out. This relates to prolongation of the plateau phase of action potential which is prolonged with hypocalcemia. Ventricular repolarization can also be long because of 1) wide QRS; 2) flat, wide T waves (e.g. quinidine, sotalol, hypokalemia, etc); and/or 3) prominent U waves melding with T wave. The latter two syndromes, representing dispersion of ventricular refractoriness, are most likely to be associated with torsade de pointes.")
30
35-yr-old: If you could only obtain one lab test what would it be
35-yr-old: If you could only obtain one lab test what would it be? * * * Difficulty ratingAnswer:Classic (!) ECG for hypercalcemia (13.9 mg/dl here). Note the very abbreviated ST segment such that the T wave looks like it takes off directly from QRS in some leads. High take-off of ST segment in V2/V3 is also sometimes seen in this context. Hypocalcemia is just the opposite: prolonged QT due to long ST segment (corresponding to changes in action potential plateau phase duration).
 ECG for hypercalcemia (13.9 mg/dl here). Note the very abbreviated ST segment such that the T wave looks like it takes off directly from QRS in some leads. High take-off of ST segment in V2/V3 is also sometimes seen in this context. Hypocalcemia is just the opposite: prolonged QT due to long ST segment (corresponding to changes in action potential plateau phase duration).")
31
51-yr-old male; what is the key ECG finding and it's differential diagnosis? * * * Difficulty ratingAnswer:The most notable finding here is a markedly prolonged QT(U) interval, best seen in the lateral precordial leads. The differential diagnosis of this important repolarization abnormality centers on 1) electrolyte disorders, especially hypokalemia and hypomagnesemia (the K+ here was at most 3.6 mEq/L, and probably lower, with a borderline low Mg++ of 1.6 mEq/L; the serum calcium was normal); and 2) drug effects (e.g., quinidine, sotalol, amiodarone, tricyclic antidepressants,etc). Hereditary long QT syndromes are much rarer. Hypocalcemia by itself stretches out the ST segment but does not produce prominent U waves. The long QT(U) with hypokalemia/hypomagnesemia is associated with an increased risk of torsade de pointes in this setting.
 electrolyte disorders, especially hypokalemia and hypomagnesemia (the K+ here was at most 3.6 mEq/L, and probably lower, with a borderline low Mg++ of 1.6 mEq/L; the serum calcium was normal); and 2) drug effects (e.g., quinidine, sotalol, amiodarone, tricyclic antidepressants,etc). Hereditary long QT syndromes are much rarer. Hypocalcemia by itself stretches out the ST segment but does not produce prominent U waves. The long QT(U) with hypokalemia/hypomagnesemia is associated with an increased risk of torsade de pointes in this setting..")
32
There is classic evidence of hyperkalemia with tall, narrow T waves, most evident in leads V3-V4, along with some QRS prolongation. These "tented T waves" are different from the broader hyperacute T waves of acute MI (usually seen with at least slight ST elevation). The low voltage is non-specific; although a pericardial syndrome is not excluded, diffuse ST elevations (due to pericarditis) or electrical alternans (a specific but not sensitive sign of tamponade when present with sinus tachycardia) are not seen. Myxedema is classically associated with sinus bradycardia and low voltage complexes ("low and slow"). The QTc interval here sec--is slightly prolonged. This may be due to the wide QRS, but also raises question of concomitant hypocalcemia in conjunction with hyperkalemia due to chronic renal failure.
. The low voltage is non-specific; although a pericardial syndrome is not excluded, diffuse ST elevations (due to pericarditis) or electrical alternans (a specific but not sensitive sign of tamponade when present with sinus tachycardia) are not seen. Myxedema is classically associated with sinus bradycardia and low voltage complexes ( low and slow ). The QTc interval here sec--is slightly prolonged. This may be due to the wide QRS, but also raises question of concomitant hypocalcemia in conjunction with hyperkalemia due to chronic renal failure..")
33
40-year-old female with life-threatening problem
40-year-old female with life-threatening problem. * * * Difficulty ratingAnswer:Hyperkalemia (associated with chronic renal failure). The K+ one hour before this ECG was 7.4 mEq/L, and likely lower at time of this tracing. Note the subtle T wave peaking ("tenting") here best seen in the lateral chest leads. Although the T waves aren't very tall, they are very narrow-based. Also present is borderline low limb lead voltage and probable left atrial abnormality.
. The K+ one hour before this ECG was 7.4 mEq/L, and likely lower at time of this tracing. Note the subtle T wave peaking ( tenting ) here best seen in the lateral chest leads. Although the T waves aren t very tall, they are very narrow-based. Also present is borderline low limb lead voltage and probable left atrial abnormality.")
35
31-year-old woman with ECG simulating ischemia
31-year-old woman with ECG simulating ischemia. What metabolic abnormality should you suspect? * * * Difficulty ratingAnswer:Hypokalemia. K+ here was 2.2mEq/L. Very severe hypokalemia can cause ST depressions and T-wave inversions as seen here, mimicking ischemia. But also note large U wave (positive deflection after ST-T and before P).
.")
36
Peaked ("tented") T waves are seen in concert with left ventricular hypertrophy (LVH), left anterior fascicular block, and very slow R-wave progression V1-V3, the latter finding raising the possibility of prior anteroseptal myocardial infarction (MI). The combination of ECG signs of hyperkalemia and LVH is strongly suggestive of underlying renal insufficiency (with hypertension to account for the LVH). The K+ here was 6.8 meq/L.
. The K+ here was 6.8 meq/L..")
37
The serum potassium was 8. 9 mEq/L
The serum potassium was 8.9 mEq/L. Note the wide QRS with tall ("peaked" or "tented") T waves in V2-V4. The PR interval is prolonged. Left atrial abnormality is also present. (Borderline right axis deviation is present which is non-diagnostic and could be due to incipient left posterior fascicular block associated with hyperkalemia or to other factors such as chronic obstructive pulmonary disease
 T waves in V2-V4. The PR interval is prolonged. Left atrial abnormality is also present. (Borderline right axis deviation is present which is non-diagnostic and could be due to incipient left posterior fascicular block associated with hyperkalemia or to other factors such as chronic obstructive pulmonary disease.")
38
The K+ was 10. 5 mEq/L in a patient with renal failure
The K+ was 10.5 mEq/L in a patient with renal failure. Note the wide QRS complexes with no evident P waves. CK was normal and ST elevations were likely due to hyperkalemia. (Note: The apparent spike after the second QRS complex is an artifact.)
")
39
The patient's serum potassium was 1
The patient's serum potassium was 1.9 mEq/L at about the time this ECG was recorded. Resting sinus tachycardia with PR prolongation is present. The P waves in lead II are superimposed on the TU waves. Marked prolongation of repolarization is present with very large U waves (V3-V4, especially). Hyperthyroidism may be associated with hypokalemic periodic paralysis, especially among Asians.
. Hyperthyroidism may be associated with hypokalemic periodic paralysis, especially among Asians.")
40
a) The ECG is very suggestive of severe hyperkalemia with the combination of symmetrically peaked T waves (V2-V4) with a wide QRS (left bundle branch block pattern here) and a long PR interval (about 0.26 sec—see lead V2). The wide QRS with severe hyperkalemia can resemble a left or right bundle branch block pattern or often shows more non-specific type of intraventricular conduction disturbance. The effects depend to some extent on any underlying conduction disturbances. Hypercalcemia produces shortening of the QT interval, which is actually prolonged here in the context of the very wide QRS. (The patient’s calcium was low at 7.6 mg/dL with a very low albumin at 1.6 gm/dL.) Severe hypothyroidism (elevated TSH) may produce sinus bradycardia and low QRS voltage. Hyponatremia does not produce distinct ECG findings. The prominent T waves raise consideration of hyperacute repolarization changes due to acute ischemia. However, the ST segments are not elevated and the T waves have a relatively narrow-based and symmetric shape very suggestive of hyperkalemia. Total CK level here was normal. The patient had ascites and renal failure with GI bleeding and probable hepatorenal syndrome, accounting for the severe hyperkalemia.
 Severe hypothyroidism (elevated TSH) may produce sinus bradycardia and low QRS voltage. Hyponatremia does not produce distinct ECG findings. The prominent T waves raise consideration of hyperacute repolarization changes due to acute ischemia. However, the ST segments are not elevated and the T waves have a relatively narrow-based and symmetric shape very suggestive of hyperkalemia. Total CK level here was normal. The patient had ascites and renal failure with GI bleeding and probable hepatorenal syndrome, accounting for the severe hyperkalemia.")
41
This ECG shows an extremely wide complex rhythm (QRS duration 0
This ECG shows an extremely wide complex rhythm (QRS duration 0.28 second) at a rate of 70 bpm. This pattern is approaching that of a so-called “sine-wave” morphology indicative of severe hyperkalemia. Atrial activity is not apparent. The patient’s serum potassium level done about ½ hr before was 6.8 mEq/L (and was likely higher at the time of this ECG). She had end-stage renal disease with a BUN of 78 mg/dL and a serum creatinine of 5.2 mg/dL. Emergency therapy of hyperkalemia is required based on this ECG finding.
 at a rate of 70 bpm. This pattern is approaching that of a so-called sine-wave morphology indicative of severe hyperkalemia. Atrial activity is not apparent. The patient’s serum potassium level done about ½ hr before was 6.8 mEq/L (and was likely higher at the time of this ECG). She had end-stage renal disease with a BUN of 78 mg/dL and a serum creatinine of 5.2 mg/dL. Emergency therapy of hyperkalemia is required based on this ECG finding.")
42
The rhythm is sinus bradycardia at a rate of about 46 bpm with prominent “J” (Osborn) waves in leads V4-V6 and marked QT prolongation (620 msec). The baseline noise in this context is consistent with shiver-related artifact. This combination of findings is virtually pathognomonic of systemic hypothermia. (The precordial voltage is borderline prominent without definite evidence of left ventricular hypertrophy.) This patient was a homeless man with no known medical history who was found unresponsive with a body temperature of 74.6 degrees F during an extremely cold spell. Laboratory findings revealed a low serum potassium level of 3.2 (normal range mEq/L) that may have contributed to the repolarization prolongation, low serum calcium of 7.3 (normal range mg/dL) proportional to the low serum albumin of 2.7 g/dL, and low normal serum magnesium 1.7 (range mg/dL). A transthoracic echocardiogram showed a normal left ventricular ejection fraction of 60 % and symmetric, diastolic left ventricular wall thickness (septum and posterior wall) at the upper limits of normal (11 mm). See also Cases 285 and 319 for comparison and further discussion. The term Osborn waves was adopted in honor of Dr. John .J. Osborn who systematically studied these hypothermia-related waves in a canine model in a classic 1953 article. For a nice write-up on this pioneering physician-scientist, see
 This patient was a homeless man with no known medical history who was found unresponsive with a body temperature of 74.6 degrees F during an extremely cold spell. Laboratory findings revealed a low serum potassium level of 3.2 (normal range mEq/L) that may have contributed to the repolarization prolongation, low serum calcium of 7.3 (normal range mg/dL) proportional to the low serum albumin of 2.7 g/dL, and low normal serum magnesium 1.7 (range mg/dL). A transthoracic echocardiogram showed a normal left ventricular ejection fraction of 60 % and symmetric, diastolic left ventricular wall thickness (septum and posterior wall) at the upper limits of normal (11 mm). See also Cases 285 and 319 for comparison and further discussion. The term Osborn waves was adopted in honor of Dr. John .J. Osborn who systematically studied these hypothermia-related waves in a canine model in a classic 1953 article. For a nice write-up on this pioneering physician-scientist, see")
43
The ECG shows a number of salient findings including: sinus tachycardia, long QT/QTc (.34 sec/.46), low limb lead and lateral QRS voltages, along with non-diagnostic slow R wave progression V1-V3 and non-specific ST-T changes. The only diagnosis listed above that accounts for the major findings is acute pancreatitis. The long QT (ST segment component is stretched out) is due to hypocalcemia (Ca mg/dL with serum albumin of 2.7 g/dL). Sinus tachycardia is due to neuroautonomic activation in this context and the low voltage is consistent with ascites/anasarca There is no evidence of acute MI by ECG and the echocardiogram was unremarkable. The literature and clinical lore suggest that both acute pancreatitis and acute cholecystitis can directly produce ECG changes exactly simulating acute MI. However, I remain skeptical of this “association” which is rare at best with two very common conditions. Finding of ST elevation in pancreatitis or cholecystitis should not be routinely attributed to the underlying abdominal pathologies and acute ischemia and related syndromes should be carefully excluded (especially: acute MI, Prinzmetal’s angina, takotsubo cardiomyopathy, ischemia due to hypotension & hypovolemic shock, etc). At the same time, systemic anticoagulation of patients with acute abdominal emergencies that occasionally are associated with ECG changes mistaken for acute STEMI can be catastrophic. p
. At the same time, systemic anticoagulation of patients with acute abdominal emergencies that occasionally are associated with ECG changes mistaken for acute STEMI can be catastrophic. p.")
44
This ECG shows sinus rhythm at a rate of about 70 bpm (there is sinus arrhythmia with a short sinus pause at the beginning). Of particular note is the shortened Q-T interval (about 280 msec) and markedly abbreviated ST segment consistent with hypercalcemia. Subtle “doming” of the ST-T complex in leads V1-V3 with slight J point/ST elevations in the right chest leads is also sometimes seen in this setting. The patient’s serum calcium at the time of this ECG was very elevated at 14.8 mg/dL (normal range ). After extensive evaluation, a diagnosis of primary hyperparathyroidism was made. For a more detailed explanation of this finding see Case # 9.
 and markedly abbreviated ST segment consistent with hypercalcemia. Subtle doming of the ST-T complex in leads V1-V3 with slight J point/ST elevations in the right chest leads is also sometimes seen in this setting. The patient’s serum calcium at the time of this ECG was very elevated at 14.8 mg/dL (normal range ). After extensive evaluation, a diagnosis of primary hyperparathyroidism was made. For a more detailed explanation of this finding see Case # 9..")
45
The clinical diagnosis was hypercalcemia (Ca++ 15
The clinical diagnosis was hypercalcemia (Ca mg/dL) due to metastatic breast cancer. The ECG shows resting sinus tachycardia with borderline left axis deviation. There is also borderline low limb lead voltage. The key finding is the very short < msec) QT interval (QT=280 msec) such that the T wave appears to take off dirrectly from the J point with marked abbreviation of the ST segment. This finding correlates with shortening of ventricular action potential [hase 2 duration. Elevation of the J point in leads V1-V2/V3 is sometimes also seen with hypercalcemia, simulating ischemia. The lower limits of the absolute QT and rate-corrected QT (QTc) intervals are not well defined, and relative shortening occurs physiologically at higher sinus rates. The two major pathologic causes of an acquired relatively short QT are hypercalcemia and digitalis glycoside effect. The latter is excluded here by the absence of characteristic "scooped" ST depressions. A hereditary form of short QT syndrome has been described recently in families with a history of sudden cardiac death bc
 due to metastatic breast cancer. The ECG shows resting sinus tachycardia with borderline left axis deviation. There is also borderline low limb lead voltage. The key finding is the very short < msec) QT interval (QT=280 msec) such that the T wave appears to take off dirrectly from the J point with marked abbreviation of the ST segment. This finding correlates with shortening of ventricular action potential [hase 2 duration. Elevation of the J point in leads V1-V2/V3 is sometimes also seen with hypercalcemia, simulating ischemia. The lower limits of the absolute QT and rate-corrected QT (QTc) intervals are not well defined, and relative shortening occurs physiologically at higher sinus rates. The two major pathologic causes of an acquired relatively short QT are hypercalcemia and digitalis glycoside effect. The latter is excluded here by the absence of characteristic scooped ST depressions. A hereditary form of short QT syndrome has been described recently in families with a history of sudden cardiac death. bc.")
46
This ECG shows classic signs of systemic hypothermia with sinus bradycardia (at about 52 beats/min), prominent J (Osborn) waves and QT prolongation (540 msec). The patient had a body temperature of 26.4 degrees C (79.5 degrees F). He also had hyperkalemia (serum K+ 6.9 mEq/L that may account for the prominent T waves superimposed on the hypothermia pattern and probably on an underlying physiologic early repolarization variant in this young adult man. For comparison and further discussion, see Case #285.
. He also had hyperkalemia (serum K+ 6.9 mEq/L that may account for the prominent T waves superimposed on the hypothermia pattern and probably on an underlying physiologic early repolarization variant in this young adult man. For comparison and further discussion, see Case #285..")
47
This ECG shows classic signs of systemic hypothermia with prominent sinus bradycardia (about 45 bpm) with marked J (Osborn) waves (see, e.g., leads V4 and V5, simulating a bundle branch block or ischemic pattern). There are also prominent T wave inversions and QT prolongation. The patient, with a history of polysubstance abuse, was found unresponsive, last seen the day before. His rectal temperature was 80.0 degrees F. Following rewarming, his ECG completely normalized. For comparison examples of typical hypercalcemia, see Cases # 9 and 67, and for tricyclic antidepressant overdose, see Case # 100. Myxedema coma is classically associated with sinus bradycardia and low voltage. (J waves have been reported with hypercalcemia but giant deflections of the type seen in this case are not a feature of hypercalcemia which may be associated with right precordial lead ST elevation (e.g., V1-V2). J waves have also been reported in subarachnoid hemorrhage, which may also be accompanied by hypothermia. In marked cases, the distinctive, convex J wave (“hypothermic hump”) appears to be an added deflection at the end of the QRS and beginning of the ST segment. The waveform is related pathophysiologically to altered transmural action potential features with hypothermia as described by the elegant work of Antzelevitch and colleagues (Circulation 1996; 93:372). Patients with this pattern are at increased risk of ventricular fibrillation which may occur during rewarming. In contrast with Brugada-type patterns (see Case 253) which are associated with “coved” (downsloping) or “saddle-back” right precordial J point/ST elevations, the hypothermic pattern is more diffuse.
. J waves have also been reported in subarachnoid hemorrhage, which may also be accompanied by hypothermia. In marked cases, the distinctive, convex J wave ( hypothermic hump ) appears to be an added deflection at the end of the QRS and beginning of the ST segment. The waveform is related pathophysiologically to altered transmural action potential features with hypothermia as described by the elegant work of Antzelevitch and colleagues (Circulation 1996; 93:372). Patients with this pattern are at increased risk of ventricular fibrillation which may occur during rewarming. In contrast with Brugada-type patterns (see Case 253) which are associated with coved (downsloping) or saddle-back right precordial J point/ST elevations, the hypothermic pattern is more diffuse.")
48
This ECG shows sinus bradycardia (52 bpm) with T wave flattening and very prominent U waves, best seen in leads V2-V3, most consistent with severe hypokalemia and/or certain types of drug effect/toxicity. The patient had marked hypokalemia. A low TSH with an elevated T4 level would be consistent with severe hyperthyroidism, which is associated with resting sinus tachycardia (or atrial fibrillation). Digoxin toxicity may be associated with sinus bradycardia but the QT interval would be relatively short. Hyponatremia and hyperchloremia are not associated with specific ECG findings. A long QT-U syndrome, hereditary or acquired, as present here, is the key ECG marker of risk for syncope or sudden cardiac death due to torsade(s) de pointes type ventricular tachycardia.
 de pointes type ventricular tachycardia.")
49
ad Sinus tachy, intraventricularis vezetési zavar, hosszú QT – QTc:670 ms – antidepresszáns túladagolás

50
Kokainista akut MI K

51
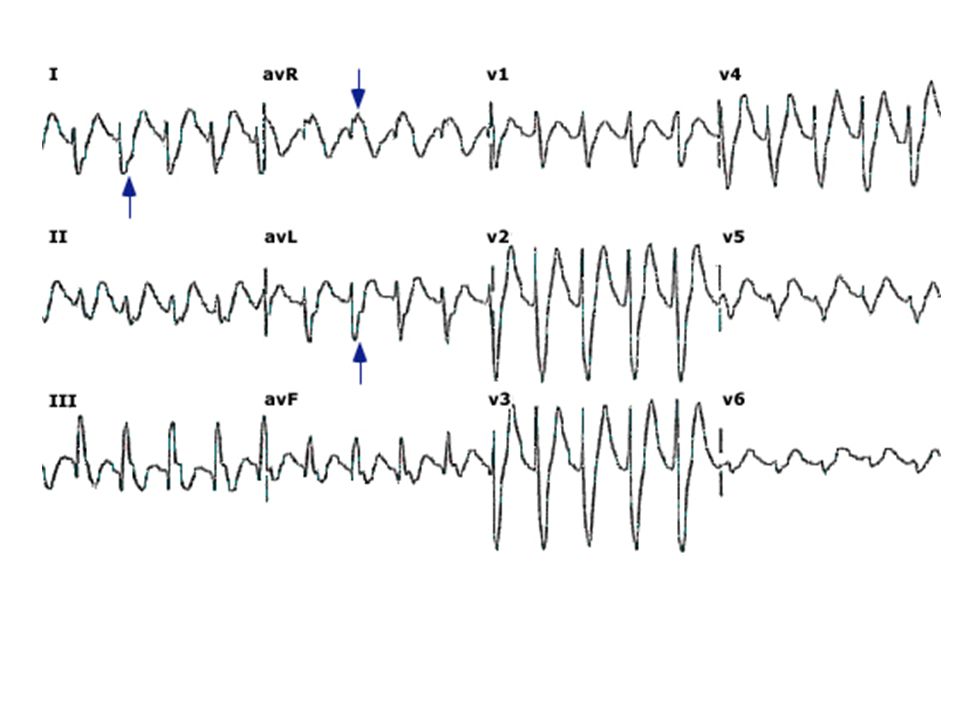
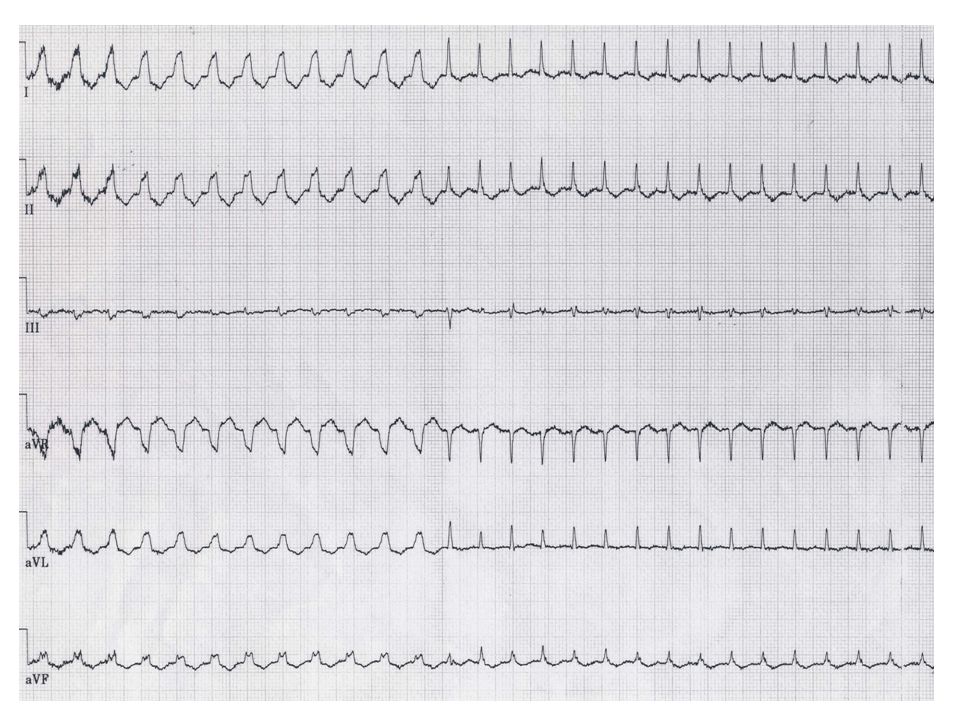
The ECG shows atrial tachycardia (atrial rate 200/min) with 2:1 AV block (ventricular rate 100/min). Look closely at V1 and you will see two distinct P waves before each QRS (one superimposed on the T wave of the preceding beat). A typical right bundle branch block (RBBB) pattern is also present with rSR’ complexes in leads VI-V3. Non-specific ST segment depressions are present. Atrial tachycardia with block should always prompt a search for digitalis toxicity, which may induce concomitant increased atrial automaticity and AV conduction impairment. One specific mechanism for the increased ectopic atrial activity may be atrial myocardial cell calcium loading due to digitalis, leading, in turn, to triggered activity from delayed afterdepolarizations. Digitalis also increases vagal tone so that the atrial tachyarrhythmia is typically combined with Type 1 AV block in this setting. Hypokalemia may play a contributory role. A digoxin level drawn the same day as this ECG was elevated at 2.3 ng/ml. It is worth noting that atrial tachycardia with AV block also often occurs in the absence of digitalis therapy due to other factors such as atrial disease, increased catecholamines, etc. Sinus rhythm with Wolff-Parkinson-White pattern is excluded as there is no evidence of a delta wave and there are 2 ectopic P waves for each QRS. Atrial flutter is excluded as there are discrete P waves and no flutter (F) waves and the atrial rate is 200 bpm (although “slow” atrial flutter with a flutter rate well below 250/min may occur especially to drugs or atrial disease). These considerations also exclude AV nodal reentrant tachycardia and monomorphic ventricular tachycardia.
 waves and the atrial rate is 200 bpm (although slow atrial flutter with a flutter rate well below 250/min may occur especially to drugs or atrial disease). These considerations also exclude AV nodal reentrant tachycardia and monomorphic ventricular tachycardia.")
52
The digoxin level was markedly elevated at 4. 2ng/ml
The digoxin level was markedly elevated at 4.2ng/ml. The ECG shows atrial fibrillation (very fine fibrillatory waves) with a slow, regularized narrow QRS rate (possible junctional escape mechanism), with multiform ventricular bigeminy. In addition, the prominent precordial voltage with a vertical QRS axis (about +90 degrees) raises consideration of underlying biventricular hypertrophy (overload). Nonspecific ST-T changes are noted, along with low QRS voltage in the limb leads. Digitalis intoxication may have myriad presentations. The combination of atrial fibrillation with a slow, regularized response and ventricular ectopy is particularly suggestive. The ventricular ectopy in such cases may be related, at least in part, to digitalis-induced calcium overload and delayed afterdepolarizations, a distinct type of triggered-activity (Rosen MR. J Am Coll Cardiol 1985; 5A:22A).
 with a slow, regularized narrow QRS rate (possible junctional escape mechanism), with multiform ventricular bigeminy. In addition, the prominent precordial voltage with a vertical QRS axis (about +90 degrees) raises consideration of underlying biventricular hypertrophy (overload). Nonspecific ST-T changes are noted, along with low QRS voltage in the limb leads. Digitalis intoxication may have myriad presentations. The combination of atrial fibrillation with a slow, regularized response and ventricular ectopy is particularly suggestive. The ventricular ectopy in such cases may be related, at least in part, to digitalis-induced calcium overload and delayed afterdepolarizations, a distinct type of triggered-activity (Rosen MR. J Am Coll Cardiol 1985; 5A:22A).")
53
The ECG shows sinus rhythm with unusual ST segment elevations/T wave inversions (“coved” pattern) in V1 and V2. This morphology and localization is strongly suggestive of a Brugada-type pattern, which may be induced by certain drugs, especially sodium channel blocking agents, in susceptible individuals. The negative enzymes, normal echocardiogram and normalization of the ECG off the epicardial bupivacaine (a reported cause of this finding) are all consistent with the diagnosis drug-induced Brugada pattern. Failure to recognize this finding could result in inappropriate therapy for ST elevation MI or to development of life-threatening ventricular arrhythmias related to the Brugada pathophysiology. See Vernooy et al. Heart Rhythm 2006;3:1074.
 are all consistent with the diagnosis drug-induced Brugada pattern. Failure to recognize this finding could result in inappropriate therapy for ST elevation MI or to development of life-threatening ventricular arrhythmias related to the Brugada pathophysiology. See Vernooy et al. Heart Rhythm 2006;3:")
54
Bónusz

60
380 ms 340 ms

Hasonló előadás











 általános mechanizmusai>")



>")




