Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Az emlőrák molekuláris genetikai osztályozásának befolyása a terápiára
Landherr László Szenológiai szimpózium 2012. november 23.

2
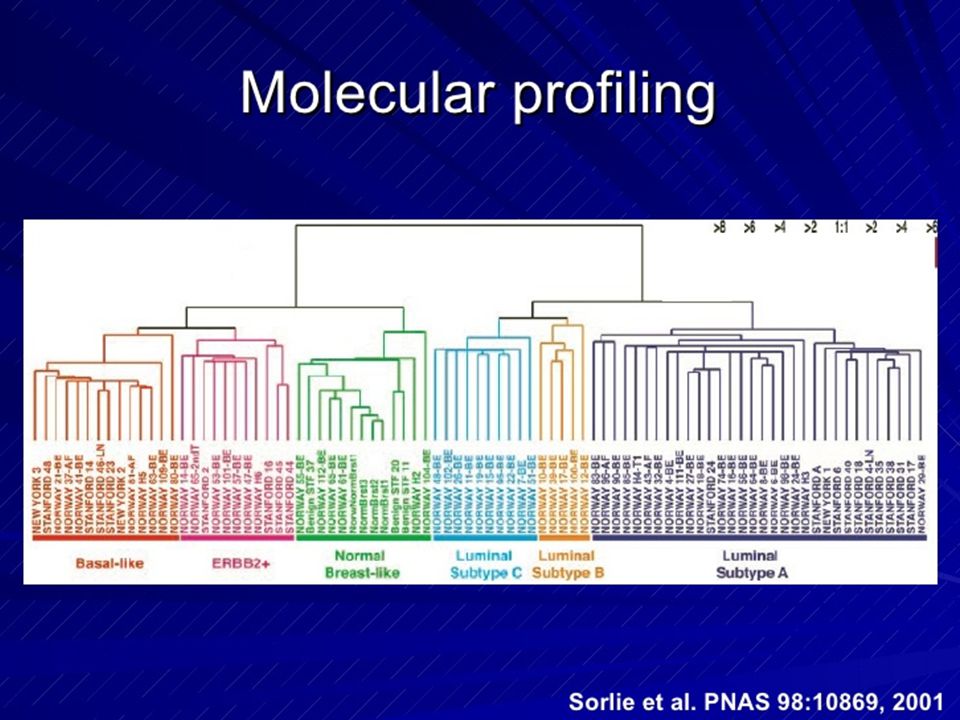
A NATURE-ben 2000-ben közölte először Sorlie és Perou, hogy az emlőtumoroknál a szubtípusok szerint különböző az adjuváns terápia hatásossága

5
gyakoriság high grade %
Luminális A (ER,PR+,HER2-) % % Luminális B (gyenge ER,PR, HER2 poz.) % % HER 2 poz % % Basal-like (Triple neg) % % (5-10% lobuláris cc.)
 52% 21% Luminális B. (gyenge ER,PR, HER2 poz.) 20% 42% HER 2 poz. 14% 62% Basal-like (Triple neg) 18% 85% (5-10% lobuláris cc.)")
6
Az adjuváns kezelés tervezése
Az emlőrák nagyon heterogén betegség A terápiás döntés alapjai ma: a tumor mérete, a grade, a nyirokcsomó státusz, ER, PR, HER2 A tumor mérete és a nyirokcsomó státusz csak prognosztikai faktorok, nem prediktívek a kezelésre adott válaszra vonatkozóan Az adjuváns kemoterápiát kapó betegeknek mindössze 2-15%-a az akiknek előnye származik a kezelésből (Lancet, 2005)
")
7
Flaherty L.E. Wayne State University

8
Molekuláris szubtípusok szerint a kemoterápiára várható válasz (%)
")
9
Molekuláris szubtípusok szerint a kemoterápiára várható válasz (%)
TAC/FAC neoadjuváns kemoterápia, RR: Basal-like 56% Luminális 3% HER2 type 50% Különböző molekuláris típusok = különböző klinikai lefolyás (pl. luminális kedvező, basal- like és HER2 kemoterápia érzékeny) PARP inhibítorok (iniparib), platina, taxánok
 PARP inhibítorok (iniparib), platina, taxánok.")
10
Az immunhisztokémiai és a molekulárisan elkülönített csoportok nem teljesen fedik egymást, pl. néhány basal-like tumor nem triple negatív és fordítva

11
A Ki67 (biomarker) szerepe a terápiás döntésben
Nukleáris non-histon protein Korrelál az ER pozitivitással Segítségével elkülöníthetők a luminális típusok 40 trial metaanalízise ( beteg): N- betegeknél enyhe prognosztikai értéke van ASCO Tumour Guidelines Commitee nem javasolja Neoadjuváns kezelésnél független prediktív faktor a pCR-re és prognosztikai a túlélésre Adjuváns CMF-re nem prediktív BIG-198: magasabb Ki67 = letrozol benefit nő ATAC: az IHC4 magasan prognosztikus értékkel bírt
: N- betegeknél enyhe prognosztikai értéke van. ASCO Tumour Guidelines Commitee nem javasolja. Neoadjuváns kezelésnél független prediktív faktor a pCR-re és prognosztikai a túlélésre. Adjuváns CMF-re nem prediktív. BIG-198: magasabb Ki67 = letrozol benefit nő. ATAC: az IHC4 magasan prognosztikus értékkel bírt.")
12
St. Galleni ajánlás a szubtípusok szerinti terápiára (2011)
Luminal A csak endokrin Luminal B (HER2 neg) endokrin ± KT Luminal B (HER2 poz) KT+anti-HER2+endokrin Non-luminal HER2 poz KT+ anti-HER2 Triple negatív (ductal) kemoterápia Spec. histológiai típusok* Hormon érzékeny endokrin terápia Nem hormon érzékeny kemoterápia Goldhirsch, et al. Annals of Oncology 22: , 2011
 endokrin ± KT. Luminal B (HER2 poz) KT+anti-HER2+endokrin. Non-luminal HER2 poz KT+ anti-HER2. Triple negatív (ductal) kemoterápia. Spec. histológiai típusok* Hormon érzékeny endokrin terápia. Nem hormon érzékeny kemoterápia. Goldhirsch, et al. Annals of Oncology 22: ,")
13
*Speciális hisztológiai típusok:
Hormon érzékeny: cribiform, tubuláris, mucinózus Nem hormon érzékeny: apocrin, medulláris, adenoid cysticus, metaplasticus Továbbra sem lehet eltekinteni a részletes morfológiai jellemzéstől

14
A gén expressziós profil alkalmazásai:
Három fő klinikai alkalmazási terület: Az emlőrák molekuláris csoportjainak elkülönítése Prognózis becslés A terápiára adott válasz jóslása (predikció)
")
15
Kell-e adni kemoterápiát az ER+, node- negatív betegeknek?
Úgy becsülhető, hogy a HR pozitív betegek közel 80–85%-a megfelelően kezelhető egyedüli endokrin terápiával. Kulcsfontosságú, hogy azonosítsuk azt a 15–20% beteget, akiknek rossz a prognózisa és valóban előnyük származik majd a kemoterápiából.

16
Proportion without distant recurrence
Az Oncotype DX® Assay prognosztikus értéke a távoli áttétek megjelenésére (NSABP B-14 Study) Távoli áttétek időben 100% 10-Year rate of recurrence = 6.8%* 95% CI: 4.0%, 9.6% 90% 80% 10-Year rate of recurrence = 14.3% 95% CI: 8.3%, 20.3% 70% 60% 10-Year rate of recurrence = 30.5%* 95% CI: 23.6%, 37.4% Proportion without distant recurrence 50% 40% All Patients, n = 668 RS < 18, n = 338 Main point: The Oncotype DX® assay is clinically validated to predict the risk of distant recurrence at 10 years in patients with ER+, node-negative breast cancer treated with tamoxifen. The Recurrence Score® result was calculated for each patient: 51% of the patient population fell into the low-risk group (n = 338), 22% fell into the intermediate-risk group (n = 149), and 27% fell into the high-risk group (n = 181). This graph demonstrates the difference in distant relapse-free survival (DRFS) over time for the different risk categories. The DRFS for the high- and low-risk groups were statistically significantly different; the 10-year distant relapse-free survival for the low-risk category was 93% compared to 69% for the high-risk category. Paik S, et al. N Engl J Med. 2004;351: 30% 20% RS 18-30, n = 149 10% RS ≥ 31, n = 181 P < 0.001 0% 2 4 6 8 10 12 14 16 RS, Recurrence Score® result Years *10-Year distant recurrence comparison between low- and high-risk groups: P < 0.001 Paik S, et al. N Engl J Med. 2004;351:
 Távoli áttétek időben. 100% 10-Year rate of recurrence = 6.8%* 95% CI: 4.0%, 9.6% 90% 80% 10-Year rate of recurrence = 14.3% 95% CI: 8.3%, 20.3% 70% 60% 10-Year rate of recurrence = 30.5%* 95% CI: 23.6%, 37.4% Proportion without distant recurrence. 50% 40% All Patients, n = 668. RS < 18, n = 338. Main point: The Oncotype DX® assay is clinically validated to predict the risk of distant recurrence at 10 years in patients with ER+, node-negative breast cancer treated with tamoxifen. The Recurrence Score® result was calculated for each patient: 51% of the patient population fell into the low-risk group (n = 338), 22% fell into the intermediate-risk group (n = 149), and 27% fell into the high-risk group (n = 181). This graph demonstrates the difference in distant relapse-free survival (DRFS) over time for the different risk categories. The DRFS for the high- and low-risk groups were statistically significantly different; the 10-year distant relapse-free survival for the low-risk category was 93% compared to 69% for the high-risk category. Paik S, et al. N Engl J Med. 2004;351: % 20% RS 18-30, n = % RS ≥ 31, n = 181. P < % RS, Recurrence Score® result. Years. *10-Year distant recurrence comparison between low- and high-risk groups: P < Paik S, et al. N Engl J Med. 2004;351:")
17
A magas RS korrelál a nagyobb haszonnal a KT-ben részesített betegeknél (NSABP B-20)
1.0 0.9 Patients with high RS 28% absolute benefit from tamoxifen + chemotherapy 0.8 0.7 0.6 Proportion without distant recurrence 0.5 N Events All patients Tamoxifen + chemotherapy Tamoxifen 424 227 33 31 P = 0.02 N Events 4.4% absolute benefit from tamoxifen + chemotherapy 0.4 Main point: The Recurrence Score® result shows that not all patients benefit equally from chemotherapy. These results recapitulate the seminal findings from the original B-20 study (Fisher B, Dignam J, Wolmark N, et al. J Natl Cancer Inst. 1997;89: ), which supported the widespread use of adjuvant cytotoxic therapy for this population. The absolute benefit of chemotherapy at 10 years is 4.4%. Is this small overall benefit due to a little benefit in many or most of the patients, or is this small benefit due to a large benefit in a subset of the patients? To address this question, the magnitude of the chemotherapy benefit was examined for each of the Recurrence Score risk groups, showing that not all women benefit equally from chemotherapy. It appears that much of the benefit associated with CMF therapy in the B-20 study was a function of the risk reduction experienced by this high-risk cohort, which represents approximately 25% of the population. The high-risk patients have a large benefit (28% absolute) from the addition of chemotherapy. This corresponds to a 74% relative risk reduction. Patients in the low-risk group (Recurrence Score value < 18) have a very low likelihood of distant recurrence. The difference between the tamoxifen alone and tamoxifen plus chemotherapy groups is not statistically significant, so the benefit of chemotherapy appears to be minimal, if any. Patients in the intermediate-risk group (Recurrence Score value 18-30), as expected, had a higher risk of distant recurrence than those in the low-risk group. The benefit of chemotherapy in the intermediate-risk patients does not appear to be large. Paik S, et al. J Clin Oncol. 2006;24: 0.3 RS < 18 Tamoxifen + chemotherapy Tamoxifen 218 135 8 4 P = 0.61 0.2 RS 18-30 Tamoxifen + chemotherapy Tamoxifen 89 45 9 4 P = 0.39 0.1 RS ≥ 31 Tamoxifen + chemotherapy Tamoxifen 117 47 13 18 P < 0.001 2 4 6 8 10 12 Years RS, Recurrence Score result Paik S, et al. J Clin Oncol. 2006;24:
, which supported the widespread use of adjuvant cytotoxic therapy for this population. The absolute benefit of chemotherapy at 10 years is 4.4%. Is this small overall benefit due to a little benefit in many or most of the patients, or is this small benefit due to a large benefit in a subset of the patients To address this question, the magnitude of the chemotherapy benefit was examined for each of the Recurrence Score risk groups, showing that not all women benefit equally from chemotherapy. It appears that much of the benefit associated with CMF therapy in the B-20 study was a function of the risk reduction experienced by this high-risk cohort, which represents approximately 25% of the population. The high-risk patients have a large benefit (28% absolute) from the addition of chemotherapy. This corresponds to a 74% relative risk reduction. Patients in the low-risk group (Recurrence Score value < 18) have a very low likelihood of distant recurrence. The difference between the tamoxifen alone and tamoxifen plus chemotherapy groups is not statistically significant, so the benefit of chemotherapy appears to be minimal, if any. Patients in the intermediate-risk group (Recurrence Score value 18-30), as expected, had a higher risk of distant recurrence than those in the low-risk group. The benefit of chemotherapy in the intermediate-risk patients does not appear to be large. Paik S, et al. J Clin Oncol. 2006;24: RS < 18. Tamoxifen + chemotherapy. Tamoxifen P = RS Tamoxifen + chemotherapy. Tamoxifen P = RS ≥ 31. Tamoxifen + chemotherapy. Tamoxifen P < Years. RS, Recurrence Score result. Paik S, et al. J Clin Oncol. 2006;24:")
18
Az Oncotype DX® Assay-vel végzett klinikai vizsgálatok eredményei ER pozitív emlőrákban
Study Design N Nodal status Prognostic Predictive NSABP B-141 Prospective; tam only 668 Neg YES - Kaiser Permanente2 Prospective; case-control 790 cases/controls NSABP B-143 Prospective; placebo vs tam 645 Quantitative ER predicts tamoxifen benefit NSABP B-204 Prospective; tam ± chemo 651 RS predicts chemotherapy benefit ECOG 21975 Prospective; AC vs AT 776 Neg/Pos SWOG 88146 367 Pos TransATAC7 Prospective; tam vs AI 1231 Main point: The Oncotype DX® assay provides reproducible results across a continuum of biology. In ER+ early-stage breast cancer, the Oncotype DX assay has been validated in numerous clinical trials to be prognostic in patients with node-negative and node-positive disease. Archived samples used in these validation studies were obtained from randomized, controlled clinical trials, not from convenience samples. In addition, the assay has been validated to predict tamoxifen and chemotherapy benefit in ER+ node-negative patients, and chemotherapy benefit in ER+ node-positive patients. Taken together, the number of clinical studies, the stringent prospective study design of these studies, and the consistency of the results in ER+ node-negative and node-positive patient populations have fulfilled the criteria of level I evidence for tumor marker studies. 1. Paik S, et al. N Engl J Med. 2004;351: 2. Habel LA, et al. Breast Cancer Res. 2006;6:R25-R39. 3. Paik S, et al. J Clin Oncol. 2005;23(16S): abstract 510. 4. Paik S, et al. J Clin Oncol. 2006; 24: 5. Goldstein LJ, et al. J Clin Oncol. 2008;26: 6. Albain KS, et al. Lancet Oncol. 2010;11:55-65. 7. Dowsett M, et al. J Clin Oncol. 2010;28: 8. Solin LJ et al, San Antonio Breast Cancer Symposium 2011; Abstract S4-6 1. Paik S, et al. N Engl J Med. 2004;351: Goldstein LJ, et al. J Clin Oncol. 2008;26: 2. Habel LA, et al. Breast Cancer Res. 2006;6:R25-R Albain KS, et al. Lancet Oncol. 2010;11:55-65. 3. Paik S, et al. J Clin Oncol. 2005;23(16S): abstract Dowsett M, et al. J Clin Oncol. 2010;28: 4. Paik S, et al. J Clin Oncol. 2006; 24:
: abstract Paik S, et al. J Clin Oncol. 2006; 24: Goldstein LJ, et al. J Clin Oncol. 2008;26: Albain KS, et al. Lancet Oncol. 2010;11: Dowsett M, et al. J Clin Oncol. 2010;28: Solin LJ et al, San Antonio Breast Cancer Symposium 2011; Abstract S Paik S, et al. N Engl J Med. 2004;351: Goldstein LJ, et al. J Clin Oncol. 2008;26: Habel LA, et al. Breast Cancer Res. 2006;6:R25-R Albain KS, et al. Lancet Oncol. 2010;11: Paik S, et al. J Clin Oncol. 2005;23(16S): abstract Dowsett M, et al. J Clin Oncol. 2010;28: Paik S, et al. J Clin Oncol. 2006; 24:")
19
Néhány, jelenleg kereskedelmi forgalomban kapható prognosztikai és prediktív genetikai teszt
Oncotype DX® MammaPrint® Mammostrat® Prognosztikus? Igen igen nem Klinikai vizsgálatban validált? Failure rate <3% 27% Nem publikálták Prediktív a kemoterápia hasznára ASCO, NCCN ajánlás St. Gallen ajánlás 1. Paik S, et al. N Engl J Med. 2004;351:2817; 2. Paik S, et al. J Clin Oncol. 2006;24:3726. 3. Bueno-de-Mesquita JM, et al. Lancet Oncol. 2007; 8: ; 4. Mook S, et al. Breast Cancer Res Treat. 2009;116:

20
Mottó: „Heterogeneity may represent tremendous opportunity for better tailoring the therapy of the patient” (Viale)
")
Hasonló előadás




















 = 100 x 0,12=12 millió Nettó eladási ár = 100+12.>")