Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

7
Overweight among children and adolescents in the USA

9
Obesity in a developing country - Gambia Prevalence (%) RuralUrban van der Sande et al (2001) in press
 RuralUrban van der Sande et al (2001) in press")
11
B/ Secondary obesity 1/ Neuroendocrine: Hypothalamic lesions, hypothyroidism, polycystic ovary syndrome, pseudohypoparathyroidism, hypogonadism, growth hormone deficiency, insulinoma, Cushing syndrome 2/ Immobility: muscular dystrophies, spina bifida, cerebral paresis, mental retardation, etc. 3/ Psychiatric diseases: depression, eating disorder, etc. 4/ Iatrogenic: Steroid treatment, sodium valproate treatment, anti-thyroid drugs and others Aetiological classification of childhood obesity

12
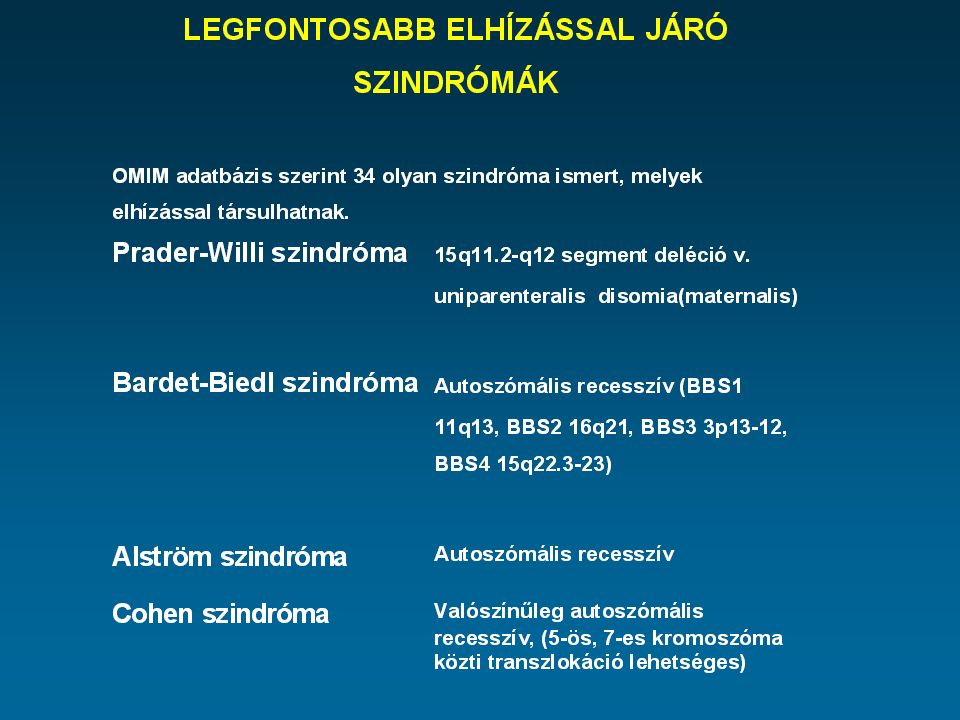
B/ Secondary obesity 5/ Genetic: Abnormalities of chromosome number: Down syndrome, Klinefelter syndrome Rare syndromes associated with obesity: There are at least 34 rare syndromes. The most frequent ones: Prader-Willi, Bardet-Biedl, Alström and Cohen syndrome Monogenic obesities: Protein convertase subtilisin type 1; Leptin; Leptin receptor; Pro- opiomelanocortin; Melanocortin 4 receptor Thyroid hormone receptor beta; Peroxisome proliferator-activated, gamma gene mutations B/ Secondary obesity 5/ Genetic: Abnormalities of chromosome number: Down syndrome, Klinefelter syndrome Rare syndromes associated with obesity: There are at least 34 rare syndromes. The most frequent ones: Prader-Willi, Bardet-Biedl, Alström and Cohen syndrome Monogenic obesities: Protein convertase subtilisin type 1; Leptin; Leptin receptor; Pro- opiomelanocortin; Melanocortin 4 receptor Thyroid hormone receptor beta; Peroxisome proliferator-activated, gamma gene mutations

15
Bardet-Biedl szindróma ÖröklődésAutoszómális recesszív (BBS1 11q13, BBS2 16q21, BBS3 3p13-12, BBS4 15q22.3-23) TermetNormál, ritkán alacsony ElhízásTeljes testre lokalizált, enyhe - súlyos fokú, 1-2 éves korban kezdődik Arc-fej diszmorfiaNem jellemző VégtagokSzámfeletti ujjak (polydactylia) Nemi szervekPrimer hipogonadizmus Mentális retardációCsökkent IQ EgyébCong. szívhiba, nefropátia, tapetoretinalis degeneráció Elhízással Járó szindrómák (2)
.")
16
Elhízással járó szindrómák (3) A lström szindróma ÖröklődésAutoszómális recesszív TermetNormál, ritkán alacsony ElhízásTörzsre lokalizált, enyhe - súlyos fokú, 2-5 éves korban kezdődik Arc-fej diszmorfiaNem jellemző VégtagokNincs eltérés Nemi szervekPrimer hipogonadizmus férfiakban, nőkben nem Mentális retardációNormál IQ EgyébAcanthosis nigricans, kopaszodás, süketség, retinitis pigmentosa
 A lström szindróma ÖröklődésAutoszómális recesszív TermetNormál, ritkán alacsony ElhízásTörzsre lokalizált, enyhe - súlyos fokú, 2-5 éves korban kezdődik Arc-fej diszmorfiaNem jellemző VégtagokNincs eltérés Nemi szervekPrimer hipogonadizmus férfiakban, nőkben nem Mentális retardációNormál IQ EgyébAcanthosis nigricans, kopaszodás, süketség, retinitis pigmentosa")
17
Elhízással járó szindrómák (4) Cohen szindróma ÖröklődésValószínűleg autoszómális recesszív, (5- ös, 7-es kromoszóma közti transzlokáció lehetséges) TermetNormál ElhízásTörzsre lokalizált, 5 éves kor körül kezdődik Arc-fej diszmorfiaMagas orrgyök, gótikus szájpad, nyitott száj, rövid filtrum VégtagokKeskeny kezek és lábak, izomhipotónia Nemi szervekNormális gonád funkciók vagy hypogonadotroph hypogonadismus Mentális retardációEnyhe EgyébDiszplasztikus fülek, pubertás késése
 Cohen szindróma ÖröklődésValószínűleg autoszómális recesszív, (5- ös, 7-es kromoszóma közti transzlokáció lehetséges) TermetNormál ElhízásTörzsre lokalizált, 5 éves kor körül kezdődik Arc-fej diszmorfiaMagas orrgyök, gótikus szájpad, nyitott száj, rövid filtrum VégtagokKeskeny kezek és lábak, izomhipotónia Nemi szervekNormális gonád funkciók vagy hypogonadotroph hypogonadismus Mentális retardációEnyhe EgyébDiszplasztikus fülek, pubertás késése")
18
Elhízással járó szindrómák (5) Carpenter szindróma ÖröklődésAutoszómális recesszív TermetNormál ElhízásTörzsre, ill. gluteális tájékra lokalizált Arc-fej diszmorfiaLapos orrgyök, gótikus szájpad, acrocephalia, exophtalmus VégtagokSzámfeletti ujjak, syndactylia, genu valgum Nemi szervekHypogonadotroph hypogonadismus Mentális retardációEnyhe Egyéb

19
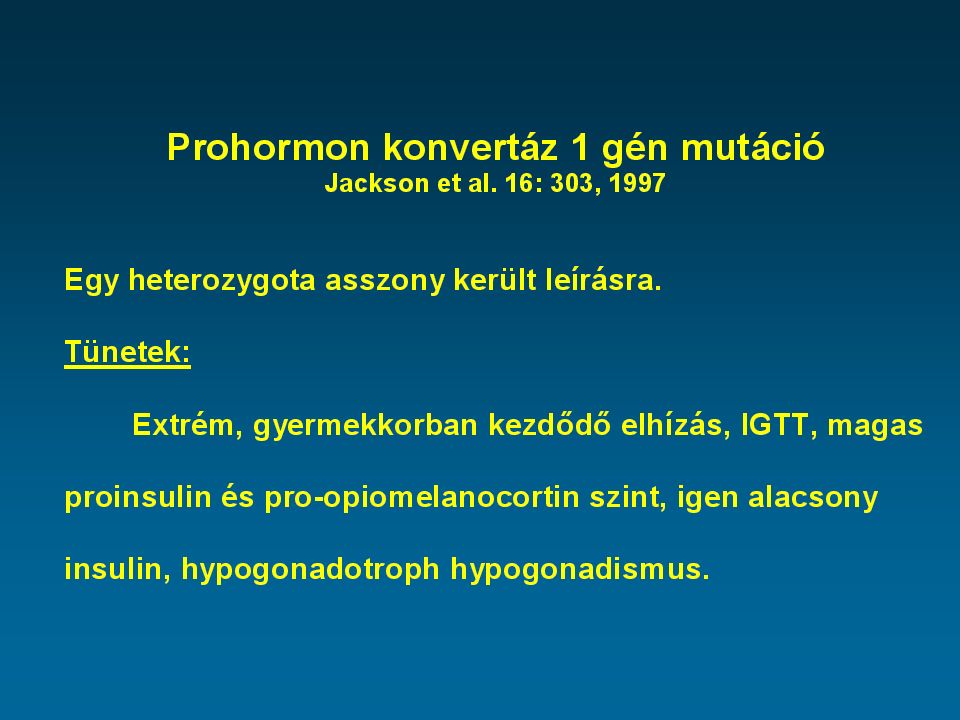
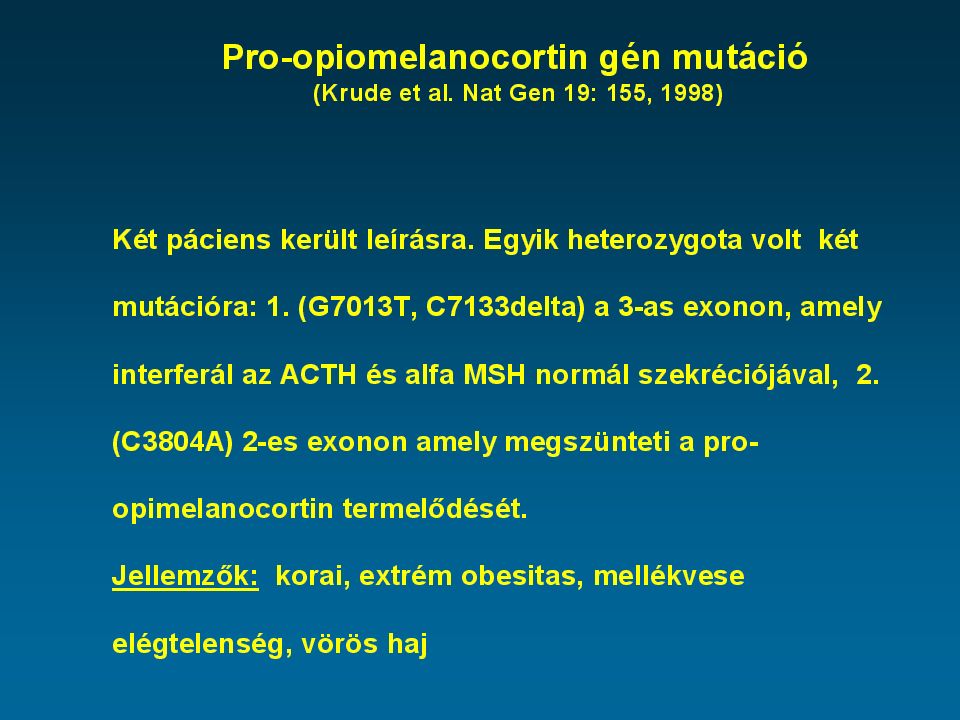
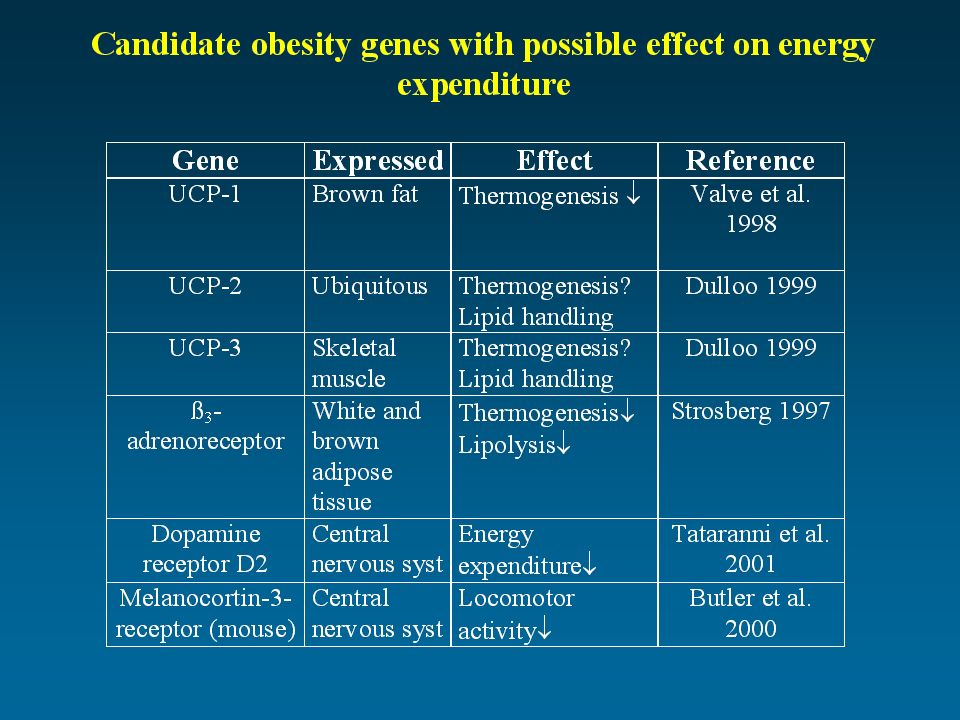
Cases of human obesity caused by single-gene mutations Pérusse L, et al. Obesity Res. 7: 11-29, 1999 Gene Location # of cases SexAgeObesity PCSK15q15-q211F3Severe LEP7q3153F, 2M2-34Severe LEPR1p313F13-19Severe POMC2p232F & M3 & 7Severe MC4R18q21.3> 95F, 4M4-78Mild to severe THBR3p24, 1-p221F15Mild PPARG3p2541F, 3M32-74Severe THBR=thyroid hormone receptor, beta PCSK1=Protein convertase subtilisin type 1 LEP=leptin, LEPR=leptin receptor; POMC=pro-opiomelanocortin PPARG=peroxisome proliferator-activated receptor, gamma MC4R=melanocortin 4 receptor

23
Production sites of Leptin White adipose tissue Brown adipose tissue Placenta Fetus Mammary epithelial cells? Stomach?

24
Leptin receptors Chorioid plexus Hypothalamus Adipose tissue ß-cells of the pancreas Lung Kidney Skeletal muscle Small intestine Prostate Testis Ovaries Placenta Fetal tissues Heart Adrenal medulla Liver

25
Functions of leptin Energy balance Pubertal dev. Reproduction Fetal dev. Angiogenesis Cellular growth Immune system Haematopoiesis

33
Ravussin et al. Diabetes Care 17: 1067-74,1994

35
Flow chart: Investigation of the obese child Obese BMI > 97% Overweight 85% < BMI < 97% BMI Family history Blood pressure Serum cholesterol Quick change of BMI Unsuccessful weight reductions in the history · Family history · Spec. history a · Body propotions, fat distribution, striae distensae b · Height, growth speed c · Minor anomalies, polydactylia, arcdysmorphia, musclehypotonia d · Development of genitalia d · Mental status d · Menstruation disturbancies, hirsutism at girls e · Bone age f · Acanthosis nigricans g Councelling Followup Poz. Neg. Detailed endocrine and/or genetic investigations Primary or „Simple” obesity Further investigations: Blood pressure OGTT (blood s glucose + insulin) Serum cholesterol, HDL-, LDL-chol., triglyceride Hepatic US, hep. function tests Neg. Poz. At risk BMI 70-85% Check BMI yearly a Head injury, headache, visual problams, vertigo ; b Cushing’s sy, Klinefelter sy; c If the child is tall or has normal stature, endocrine backgroud probably can be excluded (except Klinefelter sy); d Obesity syndromes ; e Polycystic ovarian sy; f Advanced in simple obesity, retarded in endocrine obesities t (exception: leptin deficiency); g Type 2 diabates mellitus/insulin resistance
 Serum cholesterol, HDL-, LDL-chol., triglyceride Hepatic US, hep. function tests Neg. Poz. At risk BMI 70-85% Check BMI yearly a Head injury, headache, visual problams, vertigo ; b Cushing’s sy, Klinefelter sy; c If the child is tall or has normal stature, endocrine backgroud probably can be excluded (except Klinefelter sy); d Obesity syndromes ; e Polycystic ovarian sy; f Advanced in simple obesity, retarded in endocrine obesities t (exception: leptin deficiency); g Type 2 diabates mellitus/insulin resistance.")
49
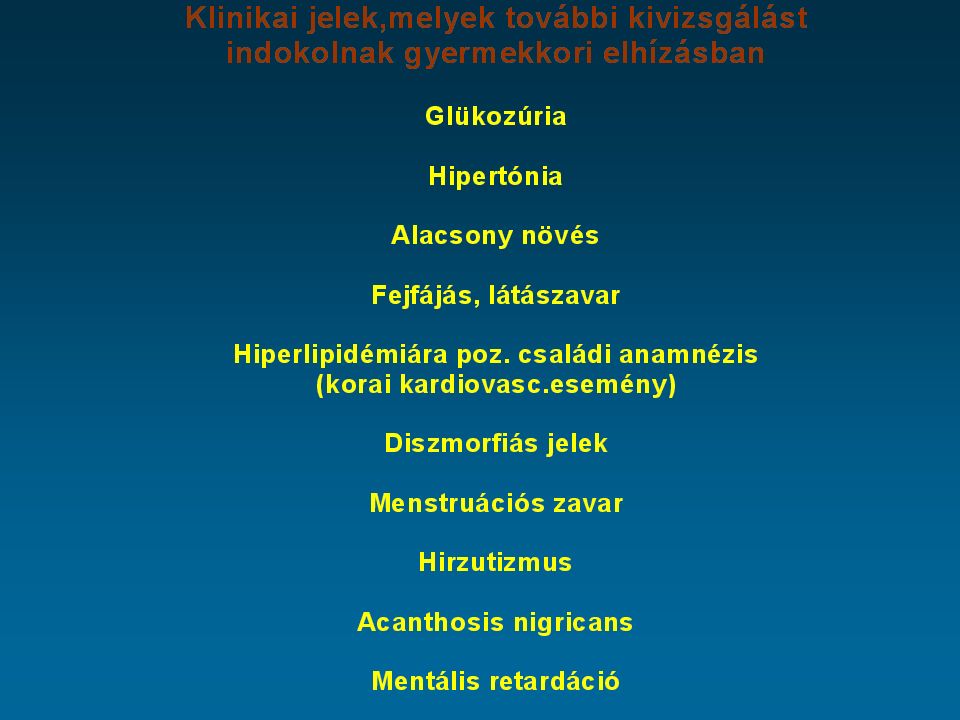
Genetikai okra kell gondolni: Korai kezdet – 6 éves kor előtt Extrem obesitas – BMI > átlag + 4SD Hyperphagia Vörös haj, mellékvese elégtelenség

52
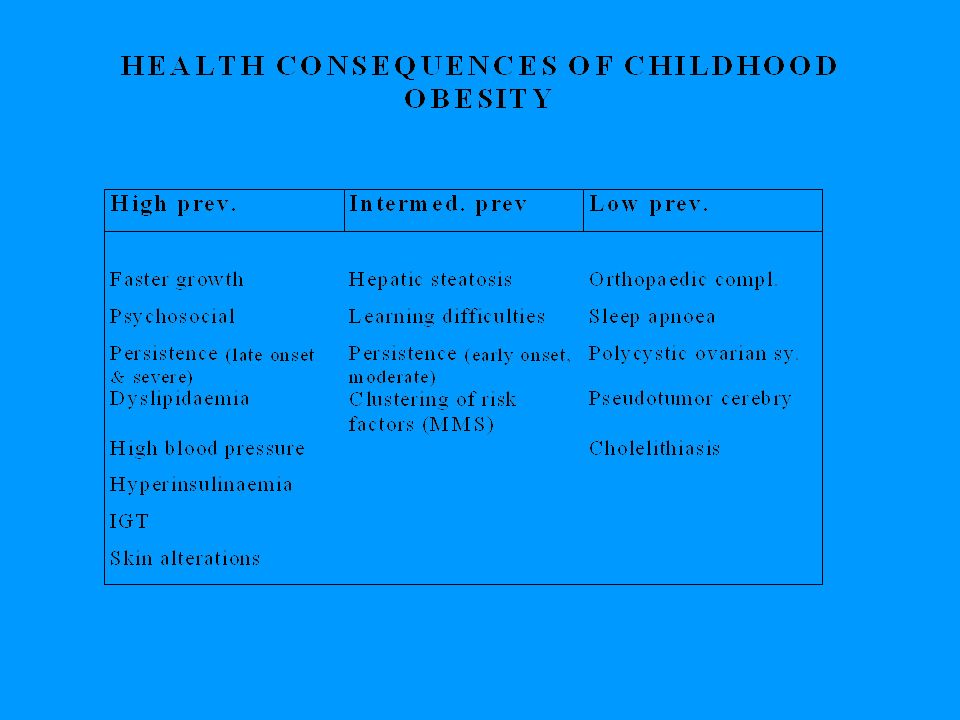
Altered physical appearance Alterations in pubertal development Physical handicap Psychosocial problems Learning difficulties Orthopaedic complications Metabolic disturbances Increased blood pressure Polycystic ovary syndrome Night hypoventilation Pseudotumor cerebri Skin alterations Immediate and intermediate consequences of childhood obesity

53
Long-term consequences of childhood obesity Obesity in adulthood Persistence of early co-morbidities Tracking of risk factors Cardiovascular disease Type 2 diabetes mellitus Hepatic steatosis and cholelithiasis Cancer Decreased socio-economic status

54
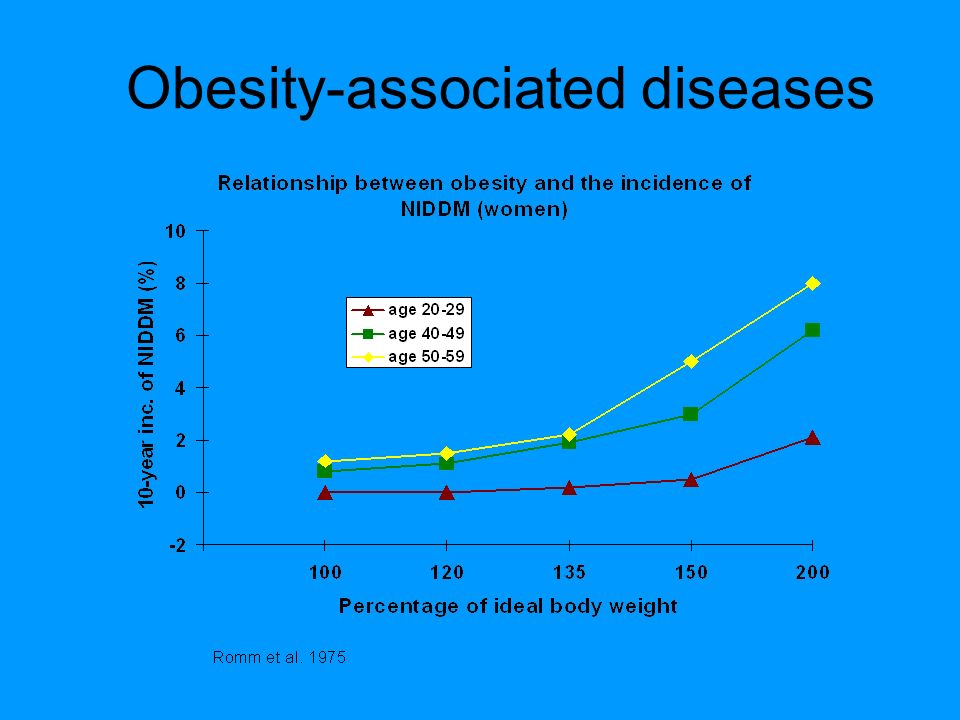
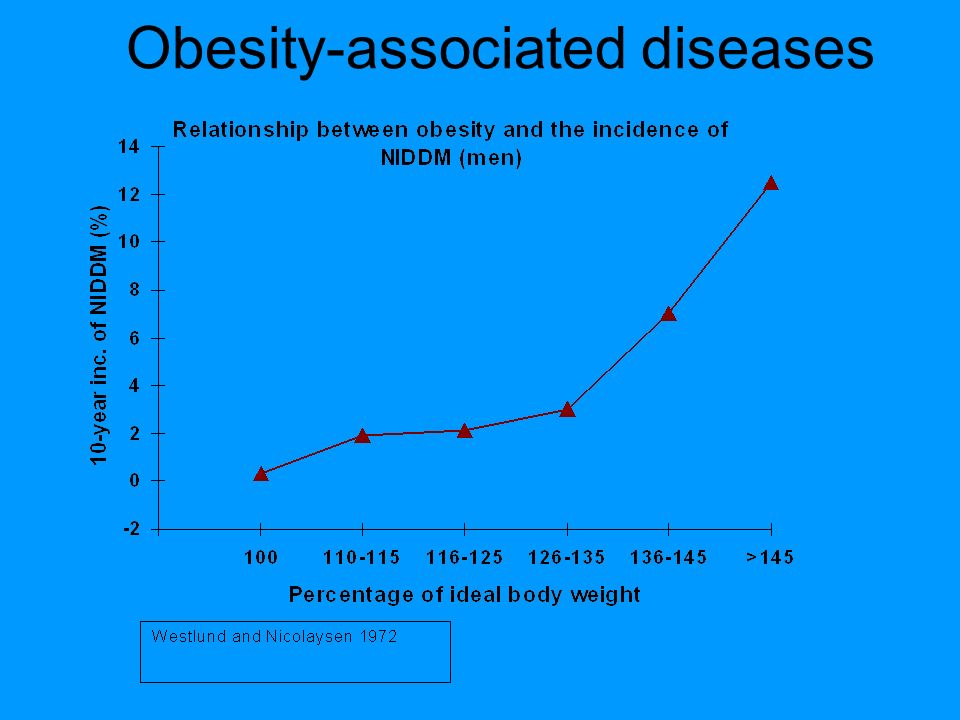
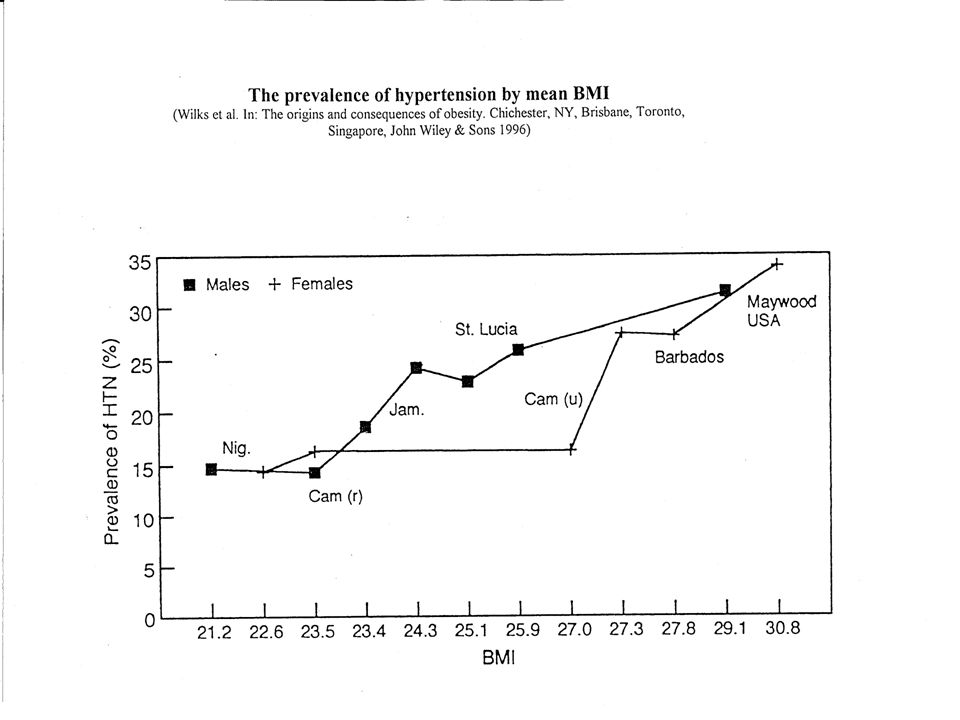
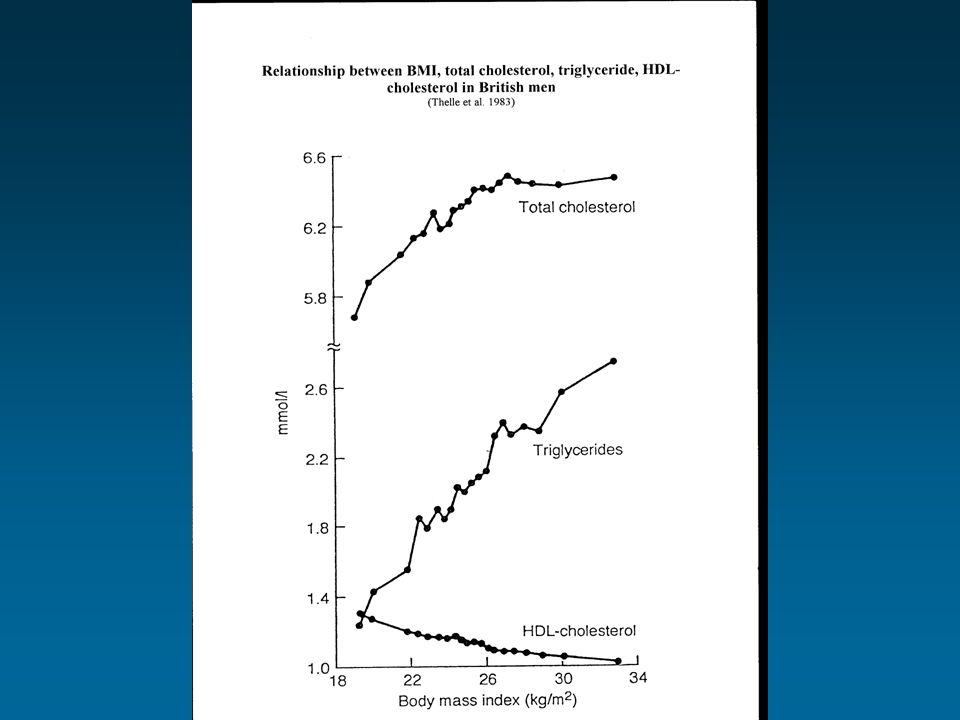
Obesity Stroke Heart disease Type 2 diabetes Osteoarthritis Sleep disorders Gout Gallbladder dis. Hypertension Some cancers Hyperlipidemia Mood disordersEating disorders Obesity-associated diseases

62
Kardiovaszkuláris rizikófaktorok

64
Relationship between mortality and BMI

65
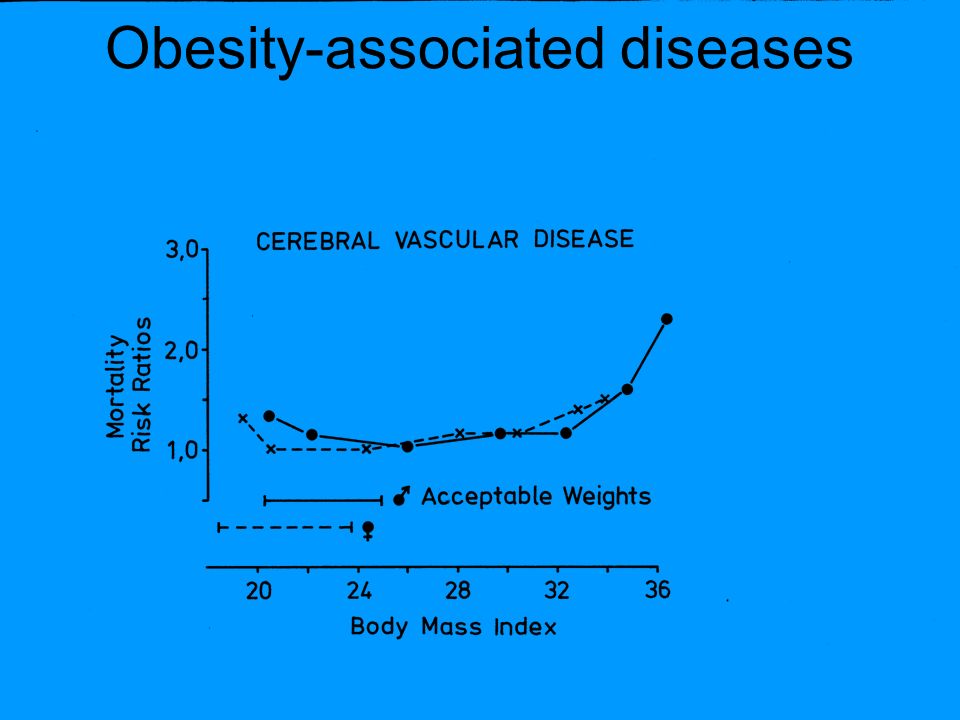
Obesity-associated diseases

73
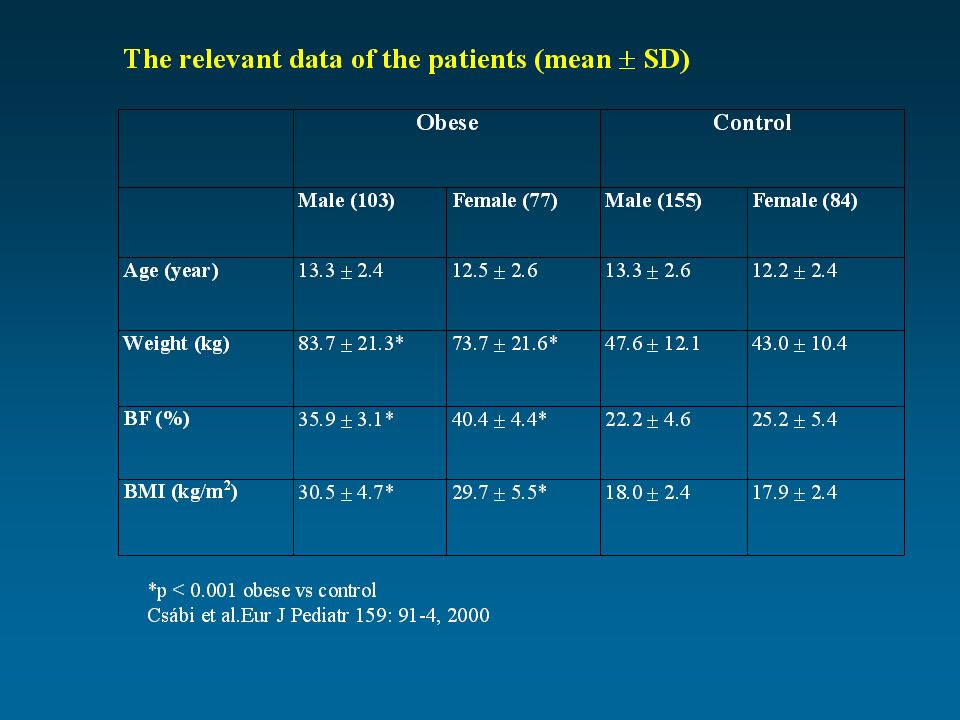
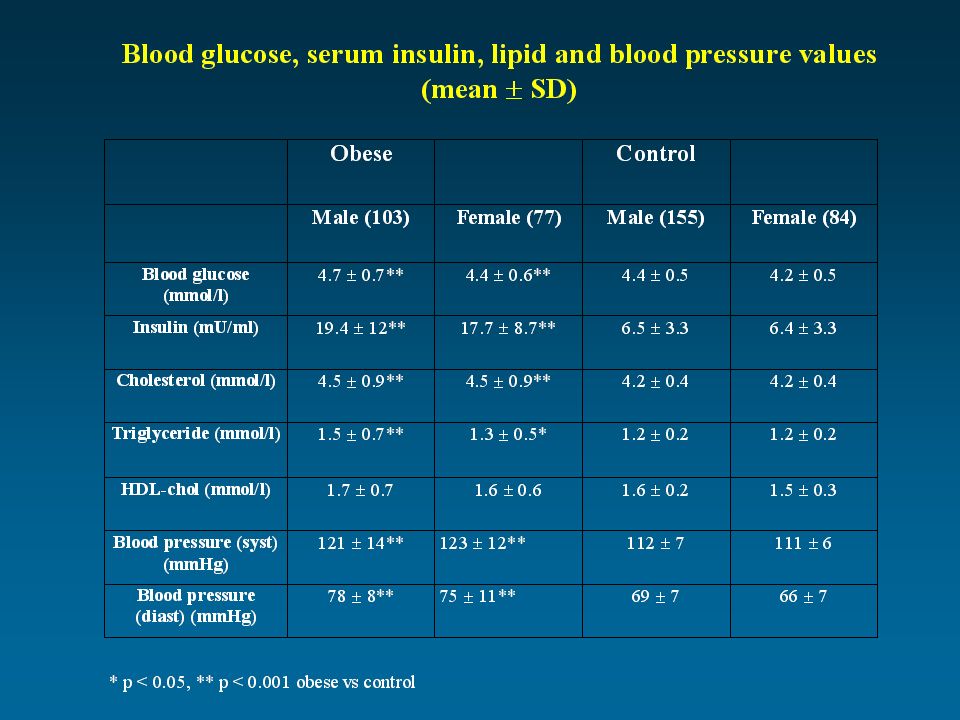
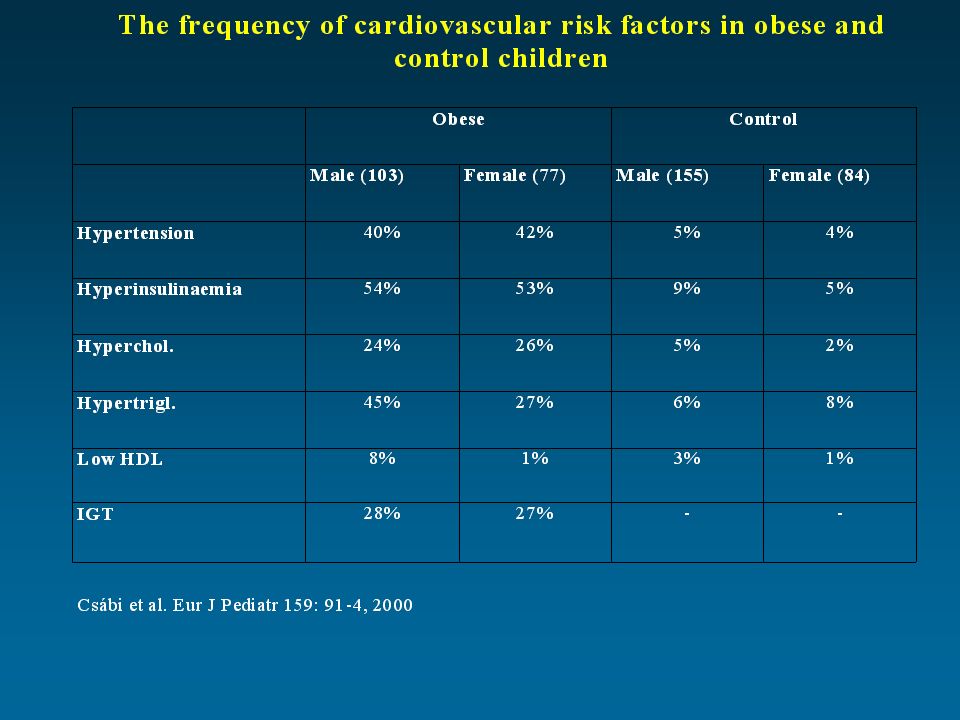
Csábi et al. Eur J Pediatr 159: 91-4, 2000

74
pmol/mmol 0 20 40 60 80 100 120 Lipid-corrected plasma ß-carotene Q1 - Q3 MMS Obese Control P<0.05 C vs Ob p<0.001 C vs MMS p<0.01 Ob vs MMS

75
mcmol/mmol 0 1 2 3 4 5 Lipid-corrected alpha-tocopherol Mean +- SD +-SD MMS Obese Control

76
mmol/l 0 0.5 1 1.5 2 2.5 Total antioxidant capacity Q1 - Q3 MMS Obese Control p<0.05, C vs. MMS and Ob vs. MMS

77
2-es típusú diabetes mellitus

78
WHO global diabetes projections Millions

79
Type II diabetes in children - Cincinnati, Ohio 10-19 year olds Rate per 100,000 19820.7 19947.2 American Diabetes Association (2000) Diabetes Care 23:381-9
 Diabetes Care 23:381-9")
80
Antropometriai adatok (átlag±SD) Összes (n=208) Fiú (n=119) Lány (n=89) Életkor (év)12,7 ± 2,812,8 ± 2,812,6 ± 2,8 Testsúly (kg)79,6 ± 21,980,7 ± 22,678,1 ± 21,0 Testmag. (cm)158,9 ± 14,7161,0 ± 16,1156,0 ± 11,9 BMI (kg/m 2 )30,9 ± 4,830,5 ± 4,231,5 ± 5,5
158,9 ± 14,7161,0 ± 16,1156,0 ± 11,9 BMI (kg/m 2 )30,9 ± 4,830,5 ± 4,231,5 ± 5,5.")
81
Szénhidrát-anyagcserezavar előfordulása Összesen: n=36 (17,3 %) IGT n= 32 (15,4 %) DM n= 4 (1,9 %) HbAlc minden esetben normális volt.
 IGT n= 32 (15,4 %) DM n= 4 (1,9 %) HbAlc minden esetben normális volt.")
82
Trp64Arg polymorphism Relationship was found: –development of type 2 diabetes mellitus –decreased RMR obesity, faster body weight increase –higher waist/hip ratio –insulin resistance –more frequent hypertension

83
Anthropometric data of children (mean±SD) and frequency of polymorphism
 and frequency of polymorphism")
84
Results of obese children (mean SD)
")
85
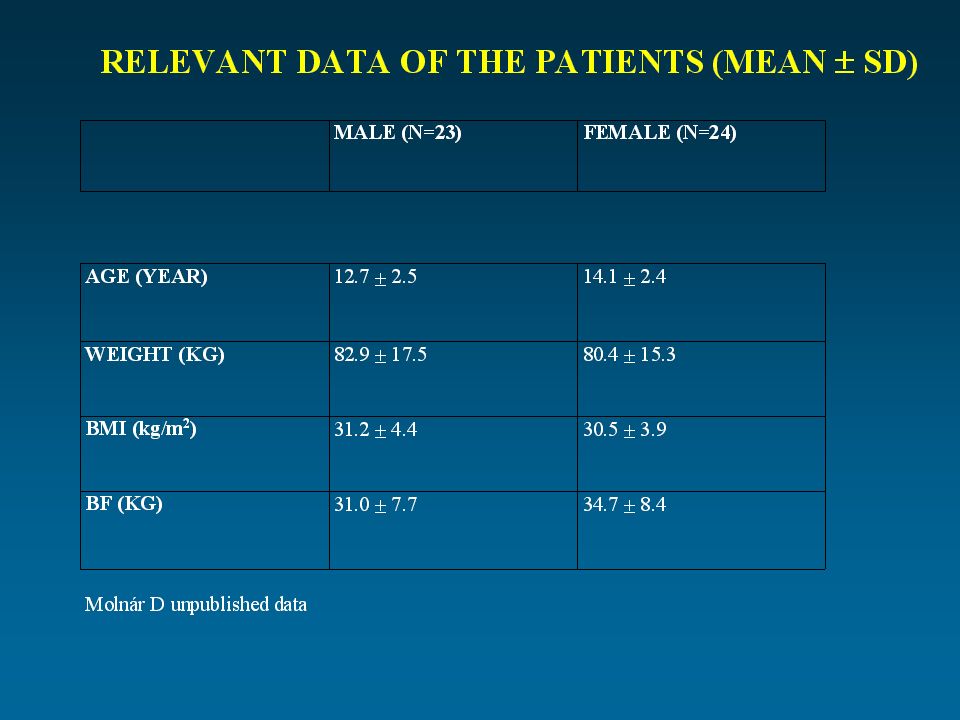
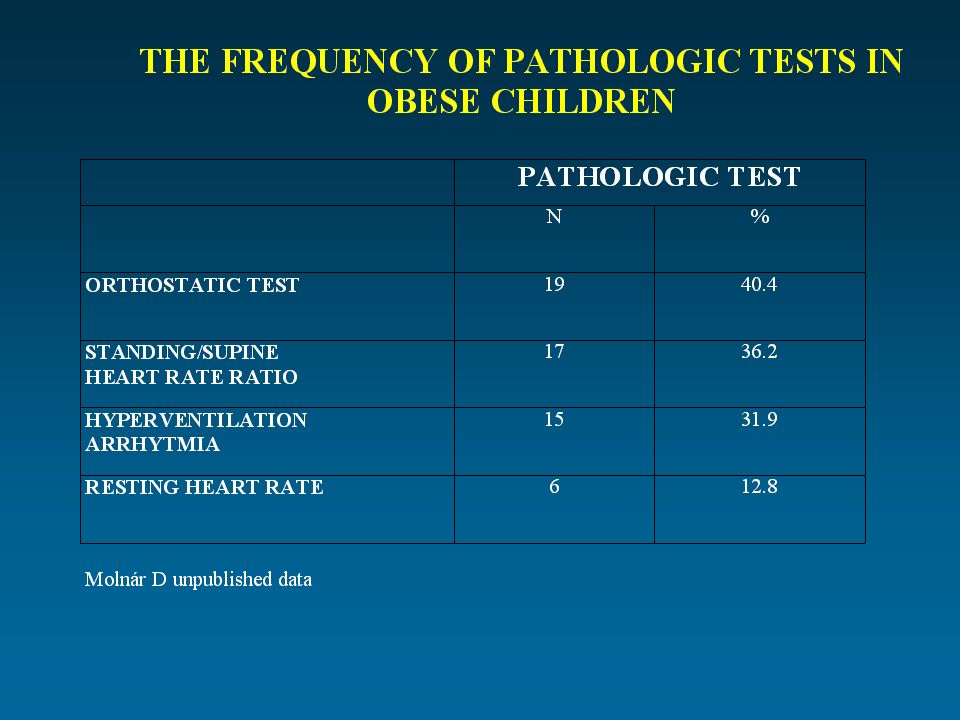
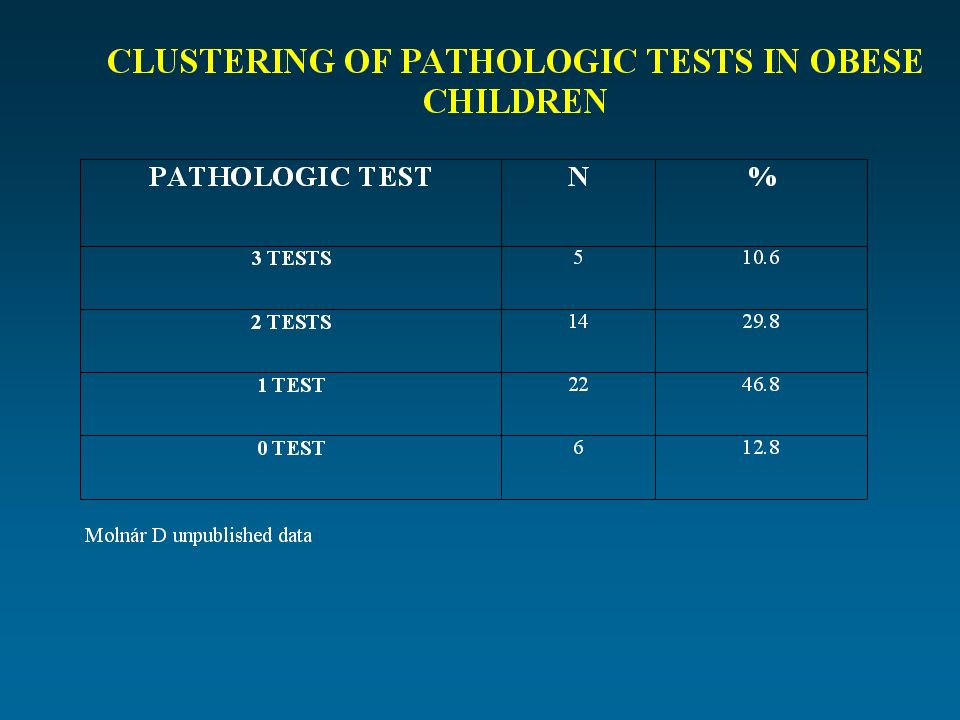
Autonom cardiovascular neuropathy in obese children

90
Következtetés A kardiovaszkuláris rizikófaktorok és azok halmozódása már gyermekkori elhízásban is észlelhető.

91
Következtetés A laboratóriumi eltérések mellett funkcionális defektusok is megjelennek elhízott gyermekbetegekben: 1/ lalacsony fizikai terhelhetőség 2/ autonom neuropátia

92
Következtetés Mindezek alapján a gyermekkori elhízás prevenciójának és a korai kezelésének jóval nagyobb hangsúlyt kellene kapnia az egészségügyben. A gyermekkori elhízás átfogó megelőzése fontos része lehetne a Nemzeti Egészségmegőrző Programnak.

97
Diéta Individualised, moderately reduced in calorie (daily energy requirement – 300-500 kCal) Low fat (< 30%) High fibre content 3-5 eatings per day
 Low fat (< 30%) High fibre content 3-5 eatings per day")
98
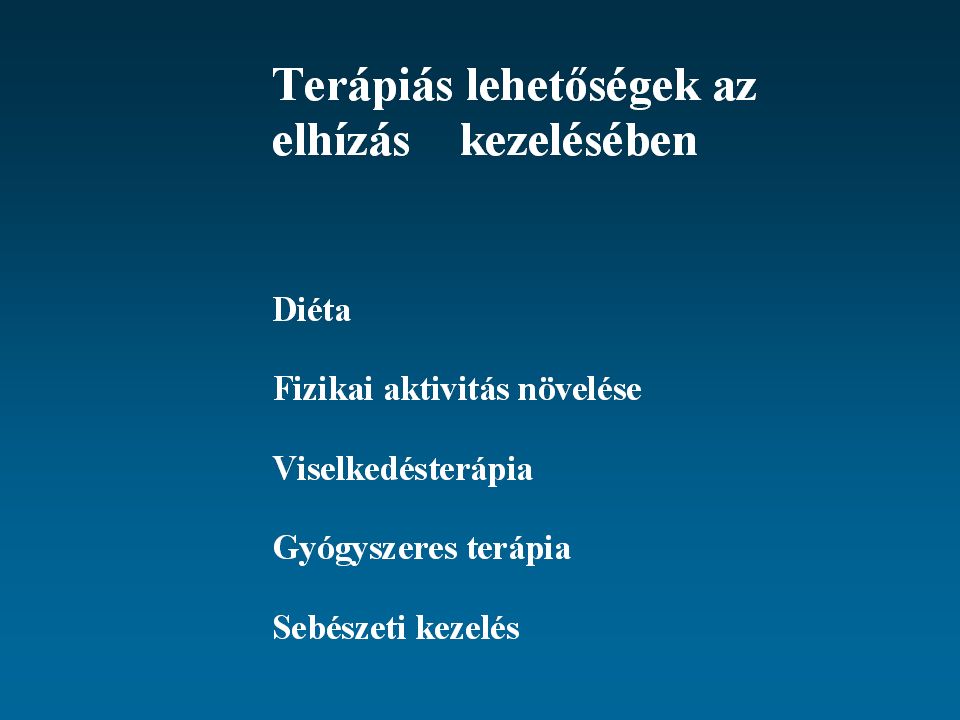
Ajánlás Összetett kezelés (diéta, fizikai aktivitás,életmódbeli változtatás,pszichoterápia, egyes esetekben gyógyszeres kezelés) Individuális kezelés Családi összefogáson alapuló Túlnyomórészt ambuláns vizsgálatok Szerény célok (a túlsúly 5-10%-os csökkentése) Hosszútávú nyomonkövetés
 Individuális kezelés Családi összefogáson alapuló Túlnyomórészt ambuláns vizsgálatok Szerény célok (a túlsúly 5-10%-os csökkentése) Hosszútávú nyomonkövetés")
Hasonló előadás































Népegészségügyi orvostan 140 és/vagy 90 Hgmm-t elérő és az.>")




