Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Légzőrendszer felső szakasza dr. Gerber Gábor

5
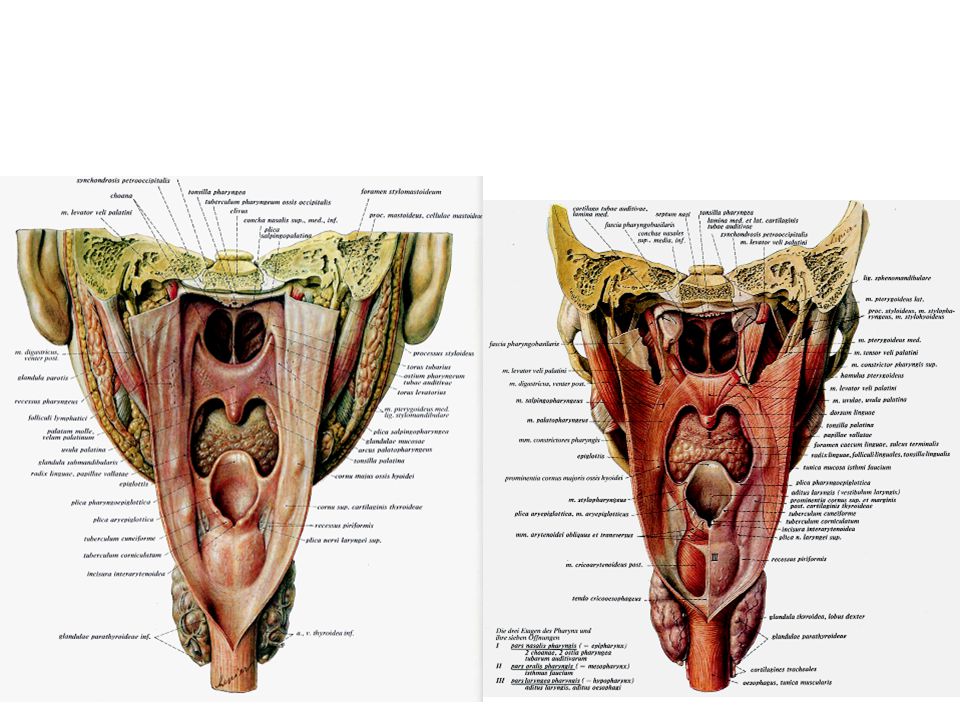
Az orrüreg összeköttetései

6
orrmelléküregek

8
A szaglóideg

9
Szaglóhámmal borított terület

10
Vomeronasalis szerv

18
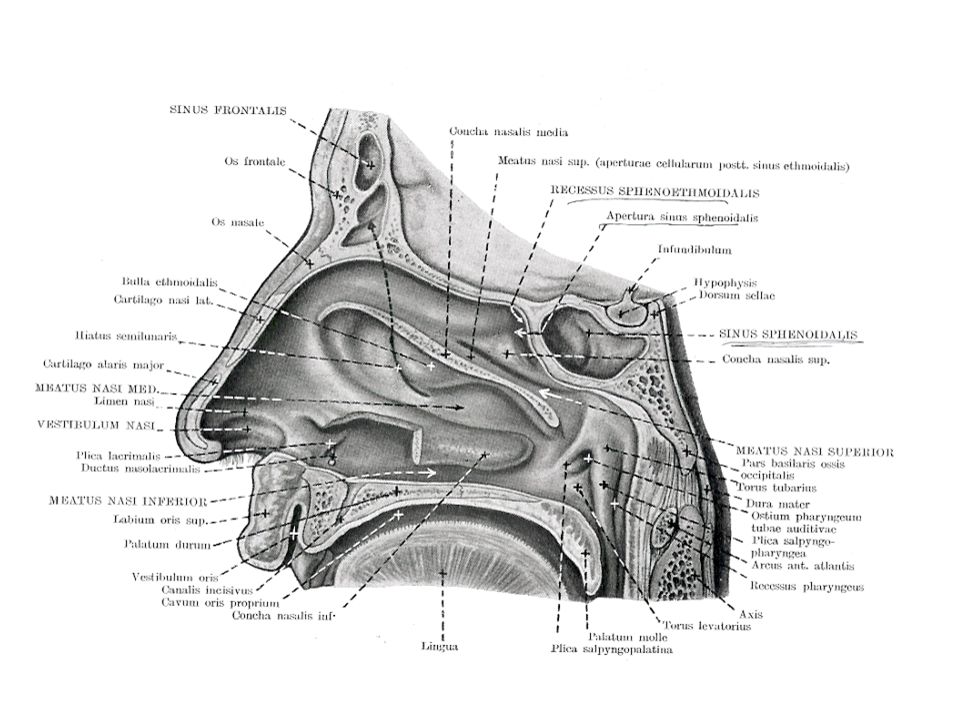
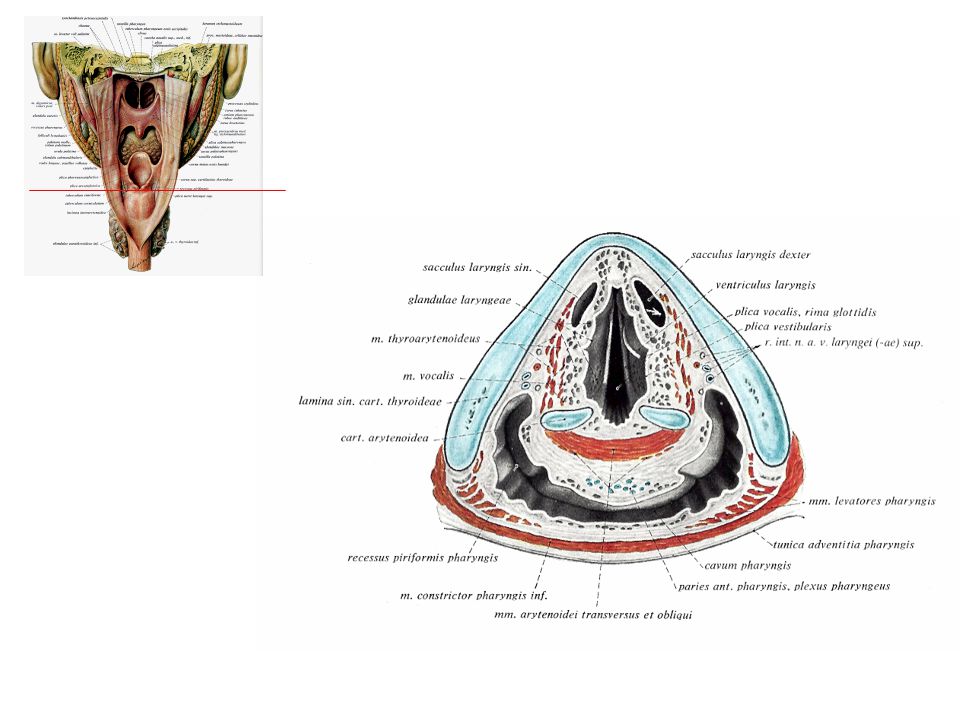
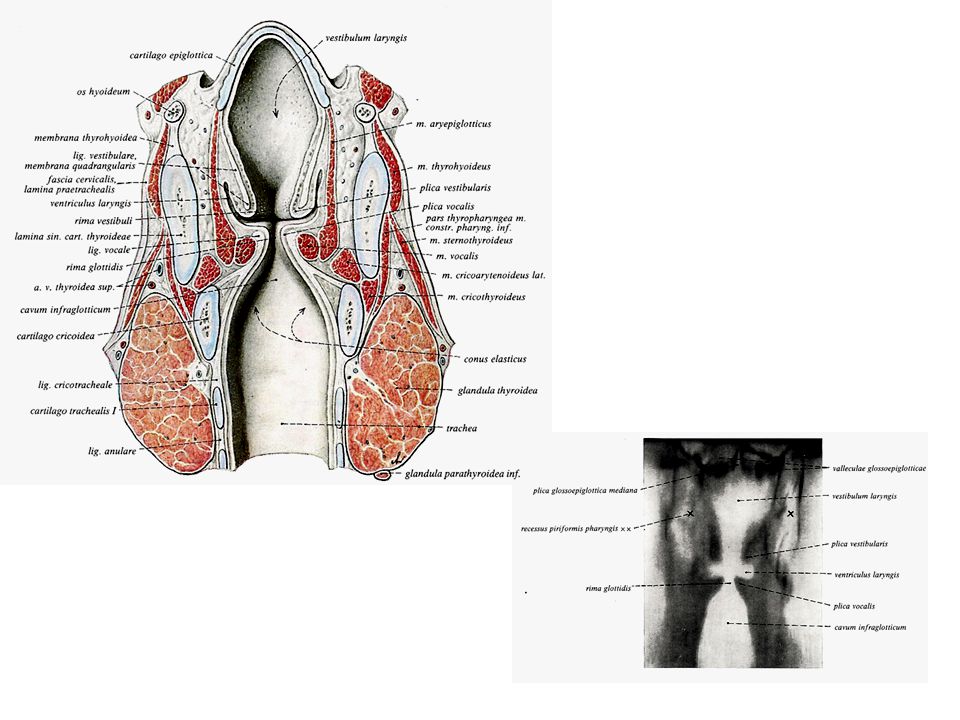
A gége sagittalis metszet

22
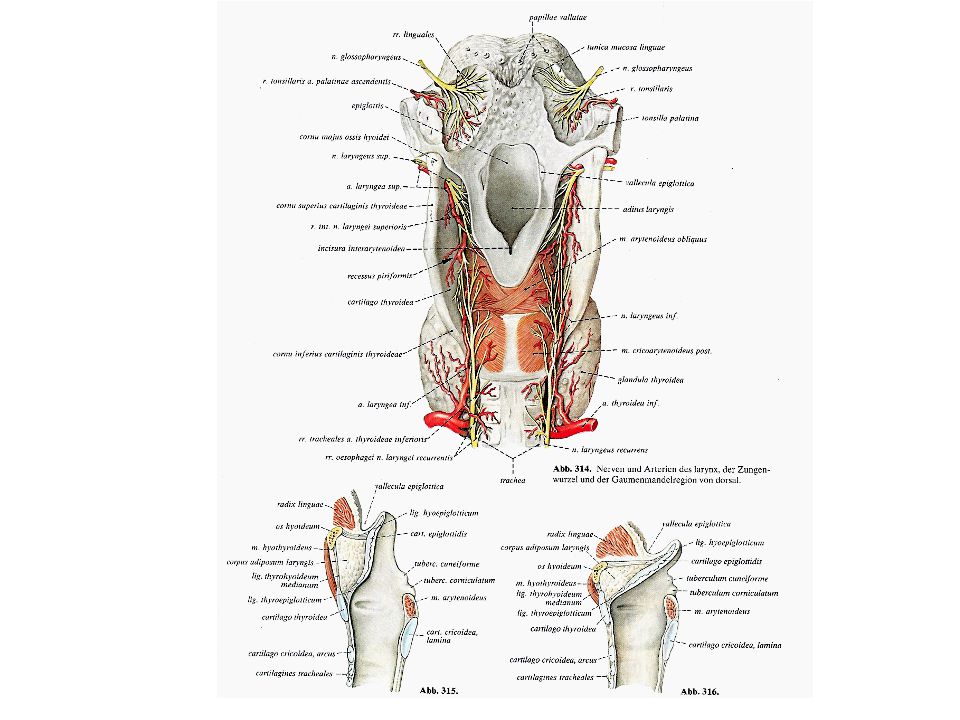
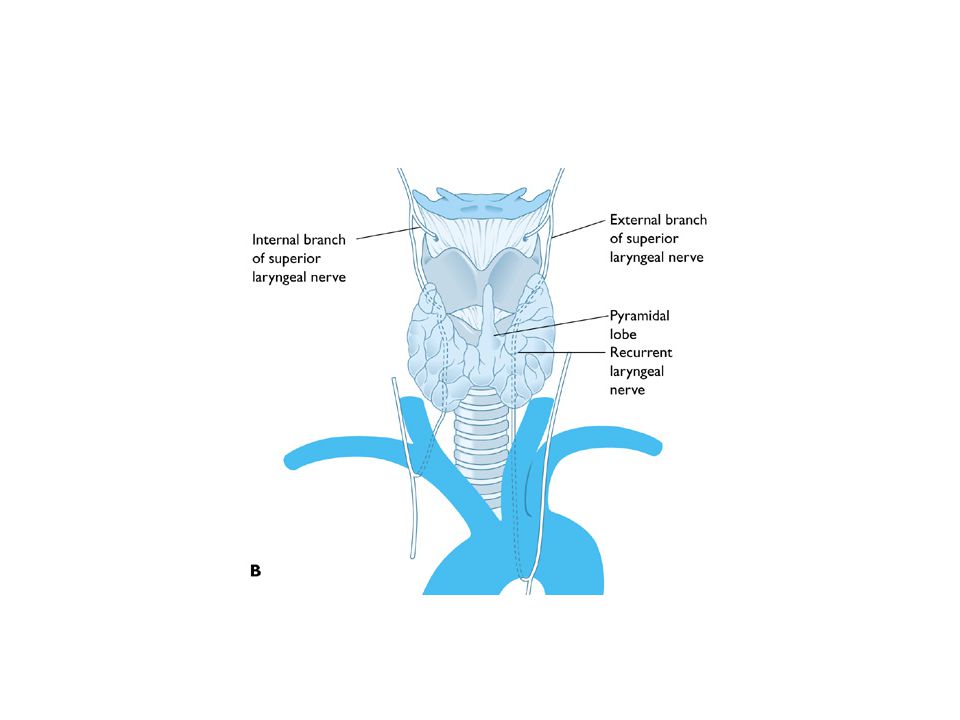
Arterial supply and venous drainage of the thyroid gland Surgical anatomy of the thyroid gland. A, Arterial supply and venous drainage of the thyroid gland. The superior and inferior thyroid arteries (STA and ITA) arise from the external carotid arteries and the thyrocervical trunks, respectively. Rarely, the thyroid ima artery, a branch from the innominate artery, may enter at the inferior margin of the thyroid isthmus. The STA is the first branch of the external carotid artery, and it has an intimate relationship with the superior laryngeal nerve, making this nerve and its motor branch, the external laryngeal nerve, susceptible to injury during thyroidectomy. The venous drainage of the thyroid gland is variable, as in other organs. The superior and middle thyroid veins drain into the internal jugular vein, and the inferior thyroid veins drain into the innominate vein. B, Anatomy of the recurrent laryngeal nerve and the superior laryngeal nerve. The external branch of the superior laryngeal nerve innervates the cricothyroid muscle, and the recurrent laryngeal nerve innervates the vocal cords. These two nerves are most susceptible to injury when dissecting, ligating, and dividing the STA and ITA at the time of thyroidectomy. Sometimes the external branch of the superior laryngeal nerve is not identified; in such cases, the STA should be ligated as close as possible to the thyroid to avoid injury to this nerve. The right recurrent laryngeal nerve takes a more oblique course as it ascends from the vagus nerve around the subclavian artery than does the left recurrent laryngeal nerve, which ascends from the vagus nerve from around the ligament arteriosum. The recurrent laryngeal nerve virtually always should be identified during thyroidectomy. It is only in 0.63% and 0.04% (right and left recurrent laryngeal nerves) of cases that this nerve does not recur because of anomalous development of the aortic arch during embryogenesis [ref].
 arise from the external carotid arteries and the thyrocervical trunks, respectively. Rarely, the thyroid ima artery, a branch from the innominate artery, may enter at the inferior margin of the thyroid isthmus. The STA is the first branch of the external carotid artery, and it has an intimate relationship with the superior laryngeal nerve, making this nerve and its motor branch, the external laryngeal nerve, susceptible to injury during thyroidectomy. The venous drainage of the thyroid gland is variable, as in other organs. The superior and middle thyroid veins drain into the internal jugular vein, and the inferior thyroid veins drain into the innominate vein. B, Anatomy of the recurrent laryngeal nerve and the superior laryngeal nerve. The external branch of the superior laryngeal nerve innervates the cricothyroid muscle, and the recurrent laryngeal nerve innervates the vocal cords. These two nerves are most susceptible to injury when dissecting, ligating, and dividing the STA and ITA at the time of thyroidectomy. Sometimes the external branch of the superior laryngeal nerve is not identified; in such cases, the STA should be ligated as close as possible to the thyroid to avoid injury to this nerve. The right recurrent laryngeal nerve takes a more oblique course as it ascends from the vagus nerve around the subclavian artery than does the left recurrent laryngeal nerve, which ascends from the vagus nerve from around the ligament arteriosum. The recurrent laryngeal nerve virtually always should be identified during thyroidectomy. It is only in 0.63% and 0.04% (right and left recurrent laryngeal nerves) of cases that this nerve does not recur because of anomalous development of the aortic arch during embryogenesis [ref]..")
25
Laryngoscope

26
Vocal Cord Paralysis ( Abductor Muscle - Strong Raspy Voice ) This video shows the function of a larynx with a left true vocal cord paralysis from a cerebral vascular accident (stroke). Note that the cord is medialized ( toward the center of the larynx ) and the voice is hoarse but strong.
 This video shows the function of a larynx with a left true vocal cord paralysis from a cerebral vascular accident (stroke). Note that the cord is medialized ( toward the center of the larynx ) and the voice is hoarse but strong.")
28
Gégemetszés

29
Heimlich fogás

30
ostium pharyngeum tubae auditivae

31
Plate 4: Eustachian Tube of Infant and Adult The infant's tube is straight and patent whereas that of the adult is angulated and closed except during the act of swallowing, yawning, etc. This factor accounts for the frequency of otitis media in early life.

32
Complicating factors in tracheal intubation in infants Complicating factors in the tracheal intubation of infants. Several differences exist between adult and infant airways (A-C) [ref]. The infant has a long, narrow nose and a long occiput. The tongue is large and predisposes to upper airway obstruction, potentially interfering with laryngoscopy and intubation. Intubation can be facilitated by placing the infant flat on the bed. Some persons place a pad under the neck to extend the head. A straight laryngoscope blade is preferred, and cricoid pressure may facilitate vocal cord exposure. In the infant (panel C), the larynx is funnel-shaped rather than cylindrical. The narrowest portion is at the cricoid ring in contrast with the adult larynx (panel B). Hence, if a tube cannot be advanced smoothly into the trachea, it should be removed and a smaller tube used. Excessive manipulation of the tube may cause tracheal damage. A—anterior; C4—fourth cervical vertebrae; P—posterior.. (Adapted from Berry [ref].)
![Complicating factors in tracheal intubation in infants Complicating factors in the tracheal intubation of infants. Several differences exist between adult and infant airways (A-C) [ref]. The infant has a long, narrow nose and a long occiput. The tongue is large and predisposes to upper airway obstruction, potentially interfering with laryngoscopy and intubation. Intubation can be facilitated by placing the infant flat on the bed. Some persons place a pad under the neck to extend the head. A straight laryngoscope blade is preferred, and cricoid pressure may facilitate vocal cord exposure.](http://slideplayer.hu/slide/2159487/8/images/32/Complicating+factors+in+tracheal+intubation+in+infants+Complicating+factors+in+the+tracheal+intubation+of+infants.+Several+differences+exist+between+adult+and+infant+airways+%28A-C%29+%5Bref%5D.+The+infant+has+a+long%2C+narrow+nose+and+a+long+occiput.+The+tongue+is+large+and+predisposes+to+upper+airway+obstruction%2C+potentially+interfering+with+laryngoscopy+and+intubation.+Intubation+can+be+facilitated+by+placing+the+infant+flat+on+the+bed.+Some+persons+place+a+pad+under+the+neck+to+extend+the+head.+A+straight+laryngoscope+blade+is+preferred%2C+and+cricoid+pressure+may+facilitate+vocal+cord+exposure..jpg "In the infant (panel C), the larynx is funnel-shaped rather than cylindrical. The narrowest portion is at the cricoid ring in contrast with the adult larynx (panel B). Hence, if a tube cannot be advanced smoothly into the trachea, it should be removed and a smaller tube used. Excessive manipulation of the tube may cause tracheal damage. A—anterior; C4—fourth cervical vertebrae; P—posterior.. (Adapted from Berry [ref].)")
33
Normal anatomy of the infant airway Normal anatomy of the infant airway. The infant airway differs from the adult in the following ways: the tongue is relatively larger, the larynx and the glottic opening are more cephalad, the epiglottis is shorter and is described as being omega-shaped, and the airway narrows from the hyoid to the level of the cricoid (A-C). Straight laryngoscope blades are more appropriate owing to the difficulty of indirectly elevating the epiglottis. The narrowing of the airway tends to form a seal around a tracheal tube, permitting the use of uncuffed tubes instead of cuffed tubes. The trachea is relatively short ranging from just less than 4 cm in a term newborn to approximately 6 cm in a 3-month-old. The short length makes proper tracheal tube placement critical to avoid bronchial intubation or accidental tracheal extubation. (From Riazi [ref]; with permission.)
. Straight laryngoscope blades are more appropriate owing to the difficulty of indirectly elevating the epiglottis. The narrowing of the airway tends to form a seal around a tracheal tube, permitting the use of uncuffed tubes instead of cuffed tubes. The trachea is relatively short ranging from just less than 4 cm in a term newborn to approximately 6 cm in a 3-month-old. The short length makes proper tracheal tube placement critical to avoid bronchial intubation or accidental tracheal extubation. (From Riazi [ref]; with permission.).")
34
drivel

35
MR images of the laryngeal air sac for the same female chimpanzee (Pal). (a) At 4 mo, a small
pouch had formed in the dorsal area of the hyoid bone. (b) At 18 mo, the sac occupied the entire area dorsal to the hyoid bone and inferior to the ventral aspect of the laryngeal cartilages. (c) At 24 mo, the sac had expanded to reach the sternum. (d) At 48 mo, the sac had expanded inferiorly into the ventral aspect of the pectoral regions and had widened at the level of the trachea. Scale in cm.
 At 18 mo, the sac occupied the entire area dorsal. to the hyoid bone and inferior to the ventral aspect of the laryngeal cartilages. (c) At 24 mo, the sac had. expanded to reach the sternum. (d) At 48 mo, the sac had expanded inferiorly into the ventral aspect of the. pectoral regions and had widened at the level of the trachea. Scale in cm.")
Hasonló előadás









. Definíció A defláció (latin: ‘lefúj’ szóból) a szél felszínalakító munkája, szűkebb és gyakrabban használt.>")
















