Előadást letölteni
1
Dyslipidemia és atherosclerosis
Dr. Pallós Júlia klinikai farmakológus – 2009.

2
A koleszterin élettani szerepe
A koleszterin a normális biológiai funkciókhoz szükséges Az összes membrán alkotórésze Szteroidok prekurzora Kortizol Progeszteron Ösztrogen Tesztoszteron Epesav A magas koleszterin-szint következménye Kardiovaszkuláris betegség Xanthomák (a bőr koleszterin-tartalmú csomói) Slide 2 Cholesterol is the “parent” steroid from which other steroids (e.g., cortisol, progesterone, estrogens, testosterone, bile acids) are derived. Cholesterol is also an important component of all cell membranes and is required for proper nervous system function.1 Excess levels of cholesterol, however, can give rise to a wide range of pathophysiologic events. The relationship between high cholesterol levels and increased risk for coronary heart disease (CHD) is well known.1,2 Very high levels of intracellular and extracellular cholesterol, as seen in patients with homozygous familial hypercholesterolemia, can also result in xanthomas (tumors consisting of foam-laden histocytes containing lipid material).3
 Slide 2. Cholesterol is the parent steroid from which other steroids (e.g., cortisol, progesterone, estrogens, testosterone, bile acids) are derived. Cholesterol is also an important component of all cell membranes and is required for proper nervous system function.1 Excess levels of cholesterol, however, can give rise to a wide range of pathophysiologic events. The relationship between high cholesterol levels and increased risk for coronary heart disease (CHD) is well known.1,2 Very high levels of intracellular and extracellular cholesterol, as seen in patients with homozygous familial hypercholesterolemia, can also result in xanthomas (tumors consisting of foam-laden histocytes containing lipid material).3.")
3
A kardiovaszkuláris betegség (KVB) rizikófaktorai
Befolyásolható Dyslipidemia emelkedett LDL alacsony HDL emelkedett TG Dohányzás Hypertónia Diabetes mellitus Elhízás Táplálkozás Thrombogén faktorok Életmód Nem befolyásolható Kor Nem Családi anamnézis Outlined here are some of the modifiable risk factors that predispose an individual to the development or progression of CHD. Evidence has shown that lifestyles associated with a “Western culture,” such as a diet rich in saturated fats and high in calories, smoking, and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CHD.1 Smoking is responsible for 50% of all avoidable deaths, half of which are due to CVD. Dyslipidemia—in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride (TG) levels, and low high-density lipoprotein (HDL) cholesterol—is associated with increased risk of CHD. However, raised LDL cholesterol has been shown to be most strongly associated with the development of atherosclerosis and the risk of CHD.1 Physicians must also be aware of the nonmodifiable risk factors for CHD such as age, sex, and family history. An in-depth family history of CHD and other atherosclerotic diseases should be an integral part of risk assessment. CHD risk is greater in males, in the elderly, and in individuals with a closely related family member with CHD. Also, the impact of any risk factor is intensified with increasing age.1 Reference Wood D, DeBacker G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: Recommendations of the Second Joint Task Force of European and Other Societies on Coronary Prevention. Atherosclerosis. 1998;140: LDL…low density lipoprotein; HDL… high density lipoprotein TG...triglycerid Wood D, et al. Atherosclerosis. 1998;140:
 cholesterol and triglyceride (TG) levels, and low high-density lipoprotein (HDL) cholesterol—is associated with increased risk of CHD. However, raised LDL cholesterol has been shown to be most strongly associated with the development of atherosclerosis and the risk of CHD.1. Physicians must also be aware of the nonmodifiable risk factors for CHD such as age, sex, and family history. An in-depth family history of CHD and other atherosclerotic diseases should be an integral part of risk assessment. CHD risk is greater in males, in the elderly, and in individuals with a closely related family member with CHD. Also, the impact of any risk factor is intensified with increasing age.1. Reference. Wood D, DeBacker G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: Recommendations of the Second Joint Task Force of European and Other Societies on Coronary Prevention. Atherosclerosis. 1998;140: LDL…low density lipoprotein; HDL… high density lipoprotein TG...triglycerid. Wood D, et al. Atherosclerosis. 1998;140:")
4
Nemzetközi KVB statisztika – férfiak 35 – 74 év
halál Koronária halál stroke halál össz halál KVB halál Bármilyen eredetű halál

5
Nemzetközi KVB statisztika – nők 35 – 74 év
KVB halál Bármilyen eredetű halál

6
Több rizikófaktor jelenléte növeli a szívinfarktus kockázatát
Nincs Csak hypertonia Csak diabetes Hypertonia + diabetes Csak dyslipidaemia Dyslipidaemia+hypertonia +/-diabetes 120 100 80 MI incidenciája* /1000 beteg 60 40 The Prospective Cardiovascular Münster Study (PROCAM) showed that rates of myocardial infarction (MI) over a 4-year follow-up period in a group of middle-aged men were increased nearly three times in people with diabetes compared with no diabetes. When diabetes mellitus and hypertension occurred together, the incidence of MI was eight-fold greater than in subjects without any risk factors. If dyslipidaemia was also present, a further two-fold increase in risk was observed. These data confirm both the independent risk associated with diabetes mellitus and the synergistic interaction that diabetes has with other common risk factors for coronary heart disease.1 Reference Assmann G, Schulte H. Am Heart J 1988;116:1713–1724. Adapted from Am Heart J 1988;116:1713–1724, with permission from Elsevier. 20 Prevalencia** (%): * Incidencia: az új esetek gyakorisága egy meghatározott időtartam alatt az eseménytől addig mentes populáció körében. ** Prevalencia: az összes létező eset előfordulása az érintett populáció körében egy meghatározott időpontban, függetlenül attól, hogy a létező eset az egyednél mióta áll fenn. Assmann G, Schulte H. Am Heart J 1988;116:1713–1724.
 showed that rates of myocardial infarction (MI) over a 4-year follow-up period in a group of middle-aged men were increased nearly three times in people with diabetes compared with no diabetes. When diabetes mellitus and hypertension occurred together, the incidence of MI was eight-fold greater than in subjects without any risk factors. If dyslipidaemia was also present, a further two-fold increase in risk was observed. These data confirm both the independent risk associated with diabetes mellitus and the synergistic interaction that diabetes has with other common risk factors for coronary heart disease.1. Reference. Assmann G, Schulte H. Am Heart J 1988;116:1713–1724. Adapted from Am Heart J 1988;116:1713–1724, with permission from Elsevier. 20. Prevalencia** (%): * Incidencia: az új esetek gyakorisága egy meghatározott időtartam alatt az eseménytől addig mentes populáció körében. ** Prevalencia: az összes létező eset előfordulása az érintett populáció körében egy meghatározott időpontban, függetlenül attól, hogy a létező eset az egyednél mióta áll fenn. Assmann G, Schulte H. Am Heart J 1988;116:1713–1724.")
7
Ép artéria felépítése Tunica adventitia Tunica media Tunica intima
Endotél (érbelhártya) Subendotelialis kötőszövet Belső elasztikus membrán Simaizom sejt Kollagén rostok Külső elasztikus membrán The normal artery has three distinct layers: the intima is the innermost layer and is composed of a single layer of endothelial cells on the luminal surface; the media is a tube of vascular smooth muscle cells (VSMCs) and their extracellular matrix; and the adventitia, the outer protective layer, is made of loose connective tissue that holds the blood vessels and nerves that supply the artery itself.1 The endothelial cells of the intima have a number of important functions: forming a nonthrombotic, nonadherent surface; acting as a semipermeable membrane; synthesizing and releasing chemical mediators; maintaining the basement membrane; and modifying lipoproteins as they cross into the artery wall.2 The VSMCs of the media contract and relax to alter the lumen diameter of the vessel in response to a variety of circulating and local stimuli, regulating vascular tone, blood flow, and blood pressure. This is caused by the production of a number of vasoactive substances, including prostaglandins, endothelin, and nitric oxide (NO).1 As the next slides reveal, LDL cholesterol is a central culprit in disrupting the normal homeostasis of the artery and its lumen, setting the stage for vascular occlusion, ischemia, and infarction. References Weissberg PL. Atherosclerosis involves more than just lipids: Plaque dynamics. Eur Heart J. 1999;1(suppl T):T13-T18. Ross R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature. 1993;362:
 Subendotelialis kötőszövet. Belső elasztikus membrán. Simaizom sejt. Kollagén rostok. Külső elasztikus membrán. The normal artery has three distinct layers: the intima is the innermost layer and is composed of a single layer of endothelial cells on the luminal surface; the media is a tube of vascular smooth muscle cells (VSMCs) and their extracellular matrix; and the adventitia, the outer protective layer, is made of loose connective tissue that holds the blood vessels and nerves that supply the artery itself.1. The endothelial cells of the intima have a number of important functions: forming a nonthrombotic, nonadherent surface; acting as a semipermeable membrane; synthesizing and releasing chemical mediators; maintaining the basement membrane; and modifying lipoproteins as they cross into the artery wall.2. The VSMCs of the media contract and relax to alter the lumen diameter of the vessel in response to a variety of circulating and local stimuli, regulating vascular tone, blood flow, and blood pressure. This is caused by the production of a number of vasoactive substances, including prostaglandins, endothelin, and nitric oxide (NO).1. As the next slides reveal, LDL cholesterol is a central culprit in disrupting the normal homeostasis of the artery and its lumen, setting the stage for vascular occlusion, ischemia, and infarction. References. Weissberg PL. Atherosclerosis involves more than just lipids: Plaque dynamics. Eur Heart J. 1999;1(suppl T):T13-T18. Ross R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature. 1993;362:")
8
Az atherosclerosis kialakulása
Hab- sejtek Korai lézió Közepes lézió Fibrózus plakk Komplikált lézió/ruptúra Atheroma Endotél diszfunkció Születés 20 évtől kezdődően 30 év felett Simaizom és kollagén Thrombosis, hematoma A növekedés elsősorban lipid akkumulációval Stary HC et al. Circulation 1995;92:

9
Az atherosclerosis klinikai tünetei
Koronária betegség Stabil angina, akut szívinfarktus (ST elevációval - STEMI,ill. ST eleváció nélkül - NONSTEMI), hirtelen halál, instabil angina Cerebrovaszkuláris betegség Stroke, TIA Perifériás artériás betegség (PAD) Intermittáló sántítás, szívinfarktus vagy stroke miatti hirtelen halál veszélye nagyobb Coronary heart disease (CHD): restriction of blood flow to the myocardium may be caused by an atherosclerotic plaque narrowing the lumen of the coronary arteries. Coronary plaque rupture and erosion may result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, myocardial infarction (MI) may occur. If damage to the myocardium is very severe, the result may be congestive heart failure or even sudden cardiac death.1 Cerebrovascular disease (CVD): narrowing of the carotid, vertebral, and cerebral arteries supplying blood to the brain can produce a transient ischemic attack (TIA) or stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture, or hemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. It can lead to permanent damage to the brain, disability, and sudden death.1 Peripheral arterial disease (PAD): when the lumen of arteries (such as the femoral and iliac, which supply blood to the legs) become sufficiently narrowed, the symptoms of intermittent claudication may become evident. These include an aching or cramping pain caused by insufficient oxygen reaching the muscles in the legs. Due to the risk of blood clots with PAD, risk of death from heart attack and stroke is increased.1 References: American Heart Association. HEART AND STROKE A–Z GUIDE. Dallas, Texas: American Heart Association, 2000. American Heart Association, 2000.
, hirtelen halál, instabil angina. Cerebrovaszkuláris betegség. Stroke, TIA. Perifériás artériás betegség (PAD) Intermittáló sántítás, szívinfarktus vagy stroke miatti hirtelen halál veszélye nagyobb. Coronary heart disease (CHD): restriction of blood flow to the myocardium may be caused by an atherosclerotic plaque narrowing the lumen of the coronary arteries. Coronary plaque rupture and erosion may result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, myocardial infarction (MI) may occur. If damage to the myocardium is very severe, the result may be congestive heart failure or even sudden cardiac death.1. Cerebrovascular disease (CVD): narrowing of the carotid, vertebral, and cerebral arteries supplying blood to the brain can produce a transient ischemic attack (TIA) or stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture, or hemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. It can lead to permanent damage to the brain, disability, and sudden death.1. Peripheral arterial disease (PAD): when the lumen of arteries (such as the femoral and iliac, which supply blood to the legs) become sufficiently narrowed, the symptoms of intermittent claudication may become evident. These include an aching or cramping pain caused by insufficient oxygen reaching the muscles in the legs. Due to the risk of blood clots with PAD, risk of death from heart attack and stroke is increased.1. References: American Heart Association. HEART AND STROKE A–Z GUIDE. Dallas, Texas: American Heart Association, American Heart Association,")
10
KVB veszélye nő, ha a nő a plazma koleszterin-szint
Framingham Study (n=5,209)2 Szérum össz koleszterin, mg/dl <204 205–234 235–264 265–294 >295 16 14 12 10 8 6 4 2 KVB Incidencia per 1,000 KVB Mortalitási ráta per 1,000 Key Point The risk of coronary heart disease (CHD) is a function of plasma cholesterol level. Additional Background Information: Hypercholesterolemia is a major modifiable factor in the development of CHD. Data from a wide variety of sources, including the Multiple Risk Factor Intervention Trial (MRFIT) and the Framingham Heart Study, have established that the risk of both CHD and CHD-related mortality increases with increasing plasma cholesterol levels.1,2 References: 1. Stamler J, Wentworth D, Neaton JD, for the MRFIT Research Group. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA. 1986;256:2823–2828. 2. Castelli WP. Epidemiology of coronary heart disease: the Framingham Study. Am J Med. 1984;76:4–12. 100 150 200 250 300 Szérum össz koleszterin, mg/dl KVB = kardiovaszkuláris betegség; MRFIT = Multiple Risk Factor Intervention Trial – klinikai vizsgálat 1. Stamler J et al. JAMA. 1986;256:2823–2828. 2. Am J Med, Vol 76, WP Castelli, Epidemiology of coronary heart disease: the Framingham Study, pp. 4–12, Copyright 1984, with permission from Excerpta Medica Inc.
2. Szérum össz koleszterin, mg/dl. < – – –294. > KVB Incidencia per 1,000. KVB Mortalitási ráta per 1,000. Key Point. The risk of coronary heart disease (CHD) is a function of plasma cholesterol level. Additional Background Information: Hypercholesterolemia is a major modifiable factor in the development of CHD. Data from a wide variety of sources, including the Multiple Risk Factor Intervention Trial (MRFIT) and the Framingham Heart Study, have established that the risk of both CHD and CHD-related mortality increases with increasing plasma cholesterol levels.1,2. References: 1. Stamler J, Wentworth D, Neaton JD, for the MRFIT Research Group. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded Findings in primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA. 1986;256:2823– Castelli WP. Epidemiology of coronary heart disease: the Framingham Study. Am J Med. 1984;76:4– Szérum össz koleszterin, mg/dl. KVB = kardiovaszkuláris betegség; MRFIT = Multiple Risk Factor Intervention Trial – klinikai vizsgálat. 1. Stamler J et al. JAMA. 1986;256:2823– Am J Med, Vol 76, WP Castelli, Epidemiology of coronary heart disease: the Framingham Study, pp. 4–12, Copyright 1984, with permission from Excerpta Medica Inc.")
11
Lipoproteinek Mivel a koleszterin, a TG és a zsírsavak vízben oldhatatlanok, a plazmában sem oldódnak. Ezért a plazmában szállítófehérjékhez (apolipoproteinek) kötődnek foszfolipidekkel együtt. Ezt a speciális komplexumot nevezik lipoproteinnek.
 kötődnek foszfolipidekkel együtt. Ezt a speciális komplexumot nevezik lipoproteinnek.")
12
Lipoproteinek fajtái A lipoproteineket a szállított zsír, a fehérje molekula (apolipoprotein) típusa és a lipoprotein nagysága alapján csoportosíthatjuk. Chylomicron VLDL (very low density lipoprotein) LDL (low density lipoprotein) HDL (high density lipoprotein)
 típusa és a lipoprotein nagysága alapján csoportosíthatjuk. Chylomicron. VLDL (very low density lipoprotein) LDL (low density lipoprotein) HDL (high density lipoprotein)")
13
Koleszterin — befolyásolható rizikófaktor!
Az össz koleszterin 10%-os csökkentése 15 %-kal csökkenti a KVB halálozás veszélyét 11 %-kal csökkenti az össz halálozás veszélyét 38 sztatin vizsgálat meta-analysise alapján 1 LDL-koleszterin az elsődleges terápiás célpont a KVB prevenciójában2 A beavatkozás intenzitása az össz kardiovaszkuláris rizikótól függ2 It has been estimated that in the United States more than 100 million adults have total cholesterol levels of 200 mg/dL and 40 million adults have levels of 240 mg/dL.1 Early lipid intervention trials have demonstrated that a reduction in total cholesterol results in a reduction in the incidence of CV events. In addition, a recent meta-analysis of 38 statin trials has shown that for every 10% reduction in total cholesterol, CHD mortality risk is reduced by 15% and total mortality risk is reduced by 11%.2 LDL cholesterol has been recognized as a prime target for lipid intervention to prevent CHD.3 Jacobson and colleagues analyzed NHANES III data and found that approximately 28.4 million Americans required drug therapy according to ATP II guidelines while only an estimated 4.5 million were receiving drug therapy.4 According to ATP III guidelines an estimated 36.5 million Americans require drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL cholesterol but also on the presence of a number of other CV risk factors.3 References American Heart Association Heart and Stroke Statistical Update. Gould AL, Rossouw JE, Santanello NC, et al. Cholesterol reduction yields clinical benefit: impact of statin trials. Circulation. 1998;97: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Jacobson TA, Griffiths GG, Varas C, et al. Impact of evidence-based "clinical judgment" on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: NHLBI. Adult Treatment Panel III (ATP III) Guidelines Slide Show. Available at: Accessed October 25, 2001. 1. Gould AL, et al. Circulation. 1998;97: 2. NCEP, Adult Treatment Panel III. JAMA. 2001;285:
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Jacobson TA, Griffiths GG, Varas C, et al. Impact of evidence-based clinical judgment on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: NHLBI. Adult Treatment Panel III (ATP III) Guidelines Slide Show. Available at: Accessed October 25, Gould AL, et al. Circulation. 1998;97: NCEP, Adult Treatment Panel III. JAMA. 2001;285:")
14
LDL koleszterin (LDL-C)
A dyslipidemia terápiájának sarokköve marad1 Szorosan összefügg az atherosclerosissal és kardiovaszkuláris eseményekkel 1 10 % emelkedése a kardiovaszkuláris rizikót 20 %-kal növeli 1 A legtöbb pácienst nem kezelik!! LDL cholesterol has been shown to be strongly associated with the development of atherosclerosis and the risk of CHD events in patients with and without established CHD. While this applies to women as well as men, the general level of CV risk is lower in premenopausal women.1 A 10% increase in LDL cholesterol is associated with an approximate 20% increase in risk for CHD.1 The association between LDL cholesterol and the risk of CV events is considerably modified by other risk factors, such as low HDL cholesterol, smoking, hypertension, and diabetes. This modification is apparent especially when total cholesterol and LDL cholesterol are only moderately elevated.1 In the US, data from NHANES indicate that most patients with elevated LDL cholesterol levels remain untreated. Upon analysis of NHANES III data Jacobson and colleagues found that approximately 28.4 million Americans required drug therapy according to ATP II guidelines while only an estimated 4.5 million were receiving drug therapy.2,3 References Wood D, De Backer G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: recommendations of the Second Joint Task Force of European and other societies on coronary prevention. Atherosclerosis. 1998;140: National Centre for Health Statistics. National Health and Nutrition Examination Survey (III) (Data collected ). Jacobson TA, Griffiths GG, Varas C, Gause D, Sung JC, Ballantyne CM. Impact of evidence-based "clinical judgment" on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: 1. Wood D et al. Atherosclerosis. 1998;140:
 (Data collected ). Jacobson TA, Griffiths GG, Varas C, Gause D, Sung JC, Ballantyne CM. Impact of evidence-based clinical judgment on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: Wood D et al. Atherosclerosis. 1998;140:")
15
HDL koleszterin (HDL-C)
Alacsony HDL-C a KVB jelentős független jelzője1 Minél alacsonyabb a HDL-C szint, annál magasabb az atherosclerosis és a KVB rizikója2 alacsony HDL-C szint: < 1 mmol/l férfiakban és 1,2 mmol/l nőkben 1 HDL-C általában alacsonyabb magas triglycerid szint esetén2 There is a strong inverse association between plasma HDL cholesterol and the risk of atherosclerosis and CHD. This effect is independent of LDL cholesterol and other risk factors.2 The higher the HDL cholesterol level, the lower the risk for atherosclerosis and CHD. Concentrations of HDL cholesterol tend to be low when triglycerides are high.2 Low concentrations of HDL cholesterol are also associated with an atherogenic lifestyle, as HDL cholesterol is lowered by smoking, obesity, and physical inactivity.2 A change in the NCEP guidelines categorically defines low HDL as a level of < 40 mg/dL as compared to the ATP II defined level of < 35 mg/dL.1 References Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Wood D, De Backer G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: recommendations of the Second Joint Task Force of European and other societies on coronary prevention. Atherosclerosis. 1998;140: 1. NCEP, Adult Treatment Panel III. JAMA. 2001;285: 2. Wood D, et al. Atherosclerosis. 1998;140:
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Wood D, De Backer G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: recommendations of the Second Joint Task Force of European and other societies on coronary prevention. Atherosclerosis. 1998;140: NCEP, Adult Treatment Panel III. JAMA. 2001;285: Wood D, et al. Atherosclerosis. 1998;140:")
16
Triglycerid Legújabb adatok azt igazolják, hogy a magas TG szint a KVB önálló rizikófaktora Normál triglycerid szint: < 150 mg/dl (1,7 mmol/l) Határérték: mg/dl (1,7 – 2,2 mmol/l) Magas: 200 to 499 mg/dl (2,2 – 5,6 mmol/l) Nagyon magas: 500 mg/dl ( 5,6 mmol/l) nő a hasnyálmirigy-gyulladás kockázata A kezelés elsődleges célja az akut pancreatitis megelőzése Hypertriglyceridemia has been shown to be associated with increased risk of CHD events; however, the association is not as strong as that of LDL cholesterol.1 Because elevated triglycerides may be considered an independent CHD risk factor, some suggest that some triglyceride-rich lipoproteins are artherogenic.2 NCEP ATP III redefines normal triglyceride levels as <150 mg/dL, borderline high 150 to 199 mg/dL, high 200 to 499 mg/dL, and very high 500 mg/dL.2 Patients with elevated triglycerides may have accompanying dyslipidemias that increase the risk for CHD (eg, familial combined hyperlipidemia, diabetic dyslipidemia, low HDL). Severe hypertriglyceridemia ( 500 mg/dL) increases the risk of pancreatitis.2 References Wood D, DeBacker G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: Recommendations of the Second Joint Task Force of European and Other Societies on Coronary Prevention. Atherosclerosis. 1998;140: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: NCEP, Adult Treatment Panel III. JAMA. 2001;285:
 Magas: 200 to 499 mg/dl (2,2 – 5,6 mmol/l) Nagyon magas: 500 mg/dl ( 5,6 mmol/l) nő a hasnyálmirigy-gyulladás kockázata. A kezelés elsődleges célja az akut pancreatitis megelőzése. Hypertriglyceridemia has been shown to be associated with increased risk of CHD events; however, the association is not as strong as that of LDL cholesterol.1 Because elevated triglycerides may be considered an independent CHD risk factor, some suggest that some triglyceride-rich lipoproteins are artherogenic.2. NCEP ATP III redefines normal triglyceride levels as <150 mg/dL, borderline high 150 to 199 mg/dL, high 200 to 499 mg/dL, and very high 500 mg/dL.2. Patients with elevated triglycerides may have accompanying dyslipidemias that increase the risk for CHD (eg, familial combined hyperlipidemia, diabetic dyslipidemia, low HDL). Severe hypertriglyceridemia ( 500 mg/dL) increases the risk of pancreatitis.2. References. Wood D, DeBacker G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: Recommendations of the Second Joint Task Force of European and Other Societies on Coronary Prevention. Atherosclerosis. 1998;140: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: NCEP, Adult Treatment Panel III. JAMA. 2001;285:")
17
Nem-HDL koleszterin = össz C – HDL-C1
Non-HDL, defined as total cholesterol minus HDL-C by ATP III, is a secondary lipid therapy target in patients with elevated triglycerides ( mg/dL). Recent data suggest elevated triglycerides are an independent CHD risk factor.1 To achieve non-HDL goals, NCEP ATP III calls for weight reduction, increased physical activity, and drug therapy. Intensified LDL-lowering drug therapy should be administered first, followed by nicotinic acid or fibrate treatment if necessary.1 References Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Cui Y, Blumenthal RS, Flaws JA, et al. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med ; 161: 1. NCEP, Adult Treatment Panel III. JAMA. 2001;285:
. Recent data suggest elevated triglycerides are an independent CHD risk factor.1. To achieve non-HDL goals, NCEP ATP III calls for weight reduction, increased physical activity, and drug therapy. Intensified LDL-lowering drug therapy should be administered first, followed by nicotinic acid or fibrate treatment if necessary.1. References. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Cui Y, Blumenthal RS, Flaws JA, et al. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med. 2001; 161: NCEP, Adult Treatment Panel III. JAMA. 2001;285:")
18
LDL- koleszterin európai/amerikai felnőtt (valószínűleg fiziológiásan)
Vadászatból élő emberek (pl. busmanok, pigmeusok, eszkimók) Újszülöttek Főemlősök Háziállatok európai/amerikai felnőtt (valószínűleg fiziológiásan) 1,3-1,9 mmol/l 0,8-1,8 mmol/l 1,0-2,1 mmol/l > 2,1mmol/l 1,3-1,8 mmol/l
 Újszülöttek. Főemlősök. Háziállatok. európai/amerikai felnőtt. (valószínűleg fiziológiásan) 1,3-1,9 mmol/l. 0,8-1,8 mmol/l. 1,0-2,1 mmol/l. > 2,1mmol/l. 1,3-1,8 mmol/l.")
19
Össz koleszterin mmol/l (mg/dl)
Európai irányelv a KVB megelőzéséről a klinikai gyakorlatban, 2007 Össz koleszterin mmol/l (mg/dl) < 4,5 mmol/l (175 mg/dl) < 4,0 mmol/l (155 mg/dl) ha megvalósítható LDL koleszterin mmol/l (mg/dl) < 2,5 mmol/l (100 mg/dl) < 2,0 mmol/l (80 mg/dl) ha megvalósítható
 < 4,5 mmol/l (175 mg/dl) < 4,0 mmol/l (155 mg/dl) ha megvalósítható. LDL koleszterin mmol/l (mg/dl) < 2,5 mmol/l (100 mg/dl) < 2,0 mmol/l (80 mg/dl) ha megvalósítható.")
20
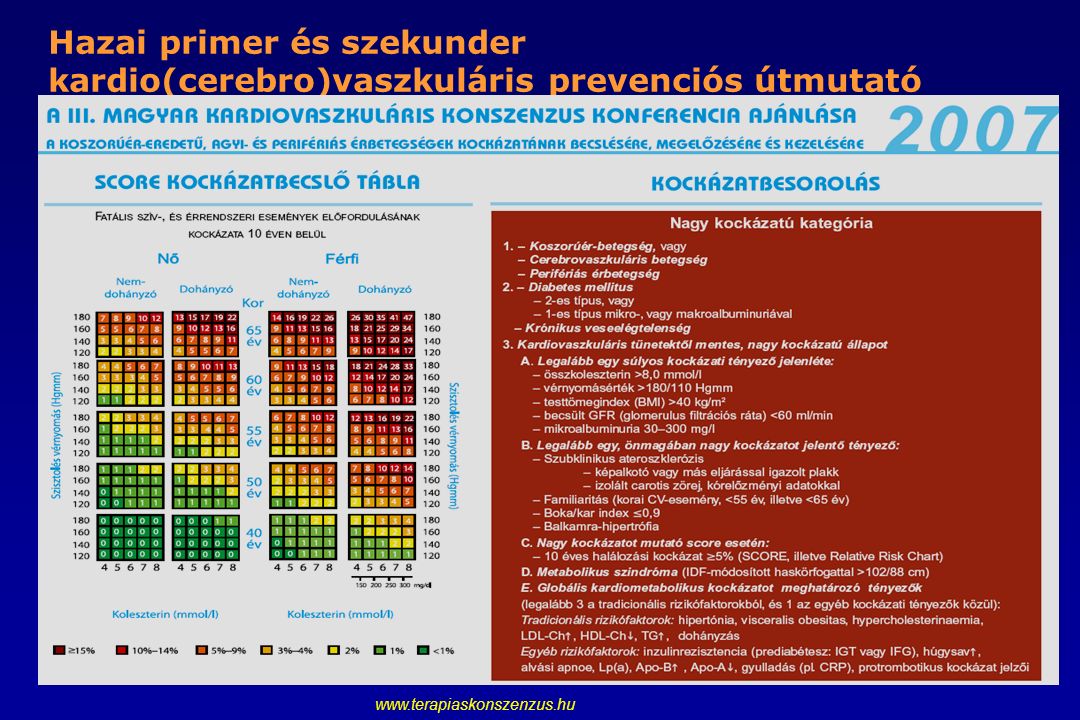
Hazai primer és szekunder kardio(cerebro)vaszkuláris prevenciós útmutató
21
Sok páciens nem éri el az LDL-koleszterin célértéket
100 90 Diéta/mozgás (%) 80 70 Gyógyszeres kezelés * (%) 70 59 60 A terápiás célértéket elérő páciensek aránya 50 40 40 30 21 20 18 10 8 The primary care Lipid Treatment Assessment Project (L-TAP) survey results showed that hypercholesterolemia treatment is suboptimal. More aggressive therapy of dyslipidemia is needed to attain NCEP goals. Results of the primary care L-TAP survey showed that hypercholesterolemia treatment is suboptimal, particularly among patients in higher risk groups. Retrospective analysis showed that only 40% of patients with two or more risk factors who were receiving various lipid-lowering drug therapies (including fluvastatin, lovastatin, pravastatin, simvastatin, gemfibrozil, bile acid sequestrants, niacin, psyllium fiber, or combination drug therapy) were meeting NCEP ATP II LDL-C goal, and only 18% of patients with CHD were meeting their NCEP LDL-C goal.1 References Pearson TA, Laurora I, Chu H, Kafonek S. The Lipid Treatment Assessment Project (L-TAP) A Multicenter Survey to Evaluate the Percentages of Dyslipidemic Patients Receiving Lipid-Lowering Therapy and Achieving Low-Density Lipoprotein Cholesterol Goals. Arch Intern Med. 2000;160: alacsony rizikó magas rizikó KVB n = 282 861 361 1924 108 1352 *sztatinok (fluvastatin, lovastatin, pravastatin, simvastatin), gemfibrozil, epesav-kötők, niacin, vagy kombinációs kezelés Adapted from Pearson TA, et al. Arch Intern Med. 2000;160:
 Gyógyszeres kezelés * (%) A terápiás célértéket elérő páciensek aránya The primary care Lipid Treatment Assessment Project (L-TAP) survey results showed that hypercholesterolemia treatment is suboptimal. More aggressive therapy of dyslipidemia is needed to attain NCEP goals. Results of the primary care L-TAP survey showed that hypercholesterolemia treatment is suboptimal, particularly among patients in higher risk groups. Retrospective analysis showed that only 40% of patients with two or more risk factors who were receiving various lipid-lowering drug therapies (including fluvastatin, lovastatin, pravastatin, simvastatin, gemfibrozil, bile acid sequestrants, niacin, psyllium fiber, or combination drug therapy) were meeting NCEP ATP II LDL-C goal, and only 18% of patients with CHD were meeting their NCEP LDL-C goal.1. References. Pearson TA, Laurora I, Chu H, Kafonek S. The Lipid Treatment Assessment Project (L-TAP) A Multicenter Survey to Evaluate the Percentages of Dyslipidemic Patients Receiving Lipid-Lowering Therapy and Achieving Low-Density Lipoprotein Cholesterol Goals. Arch Intern Med. 2000;160: alacsony rizikó. magas rizikó. KVB. n = *sztatinok (fluvastatin, lovastatin, pravastatin, simvastatin), gemfibrozil, epesav-kötők, niacin, vagy kombinációs kezelés. Adapted from Pearson TA, et al. Arch Intern Med. 2000;160:")
22
Mi nehezíti a koleszterin célértékek elérését?
Páciens / Orvos-függő faktorok A magas koleszterin-szintet nem diagnosztizálják vagy nem kezelik A gyógyszer adagolása nem megfelelő Rossz utánkövetés Páciens rossz gyógyszerszedési hajlandósága Slide 10 Patients may not achieve LDL goals for many reasons. Culpability can be related to failings by patients and their physicians as well as to limitations of currently available drugs. The most important reason, however, is that hypercholesterolemia is often underdiagnosed and either untreated or undertreated.28,29 Treatment is further compromised by poor follow-up of patients to ensure achievement of goals.28 Poor adherence to potentially effective therapy is another reason why LDL goals may remain unmet.28 Available lipid-lowering drugs, while effective and well tolerated in many patients, also have limitations. Interpatient variability marks the response to statins, and some individuals may experience hepatotoxic effects or elevated muscle enzymes. Tolerability-limiting adverse effects of nicotinic acid include flushing, gastrointestinal events, and pruritus. Bile acid-binding resins are poorly palatable and produce gastrointestinal side effects.21 Gemfibrozil may be prothrombotic by increasing both platelet number and aggregability.30 Olson KL et al Pharmacotherapy 2001;21: ; Straka RJ et al Pharmacotherapy 2001;21: ; lllingworth DR Med Clin North Am 2000;84:23-42; Broijersen A et al Arterioscler Thromb Vasc Biol 1995;15:

23
A hyperlipidemia kezelése
Magas LDL-C Életmód megváltoztatása Treatment of hyperlipidemia Statins have been and remain the drugs of first choice for lowering LDL-C. They lower LDL-C more effectively than other currently available agents, and they reduce CHD risk. Because of their LDL-C–lowering efficacy, they are able to achieve LDL-C treatment goals in the majority of patients, regardless of their risk category. In fact, the more potent the LDL-C–lowering efficacy of the statin, the greater the percentage of patients who will achieve their LDL-C goal. Statins are also remarkably safe as will be described below. About 5–10% of patients will not be able to tolerate a statin and so the only alternative agents for lowering LDL-C are a bile acid resin and niacin. These drugs are not as effective in lowering LDL-C and cause bothersome side effects which make patient compliance a problem. However, they are effective in reducing CHD risk and in the majority of patients can be successfully taken. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Gyógyszerek Választandó: Sztatin Alternatíva: ezetimib, niacin
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Gyógyszerek. Választandó: Sztatin. Alternatíva: ezetimib, niacin.")
24
Kevert hyperlipidemia kezelése
Magas LDL-C és TG Életmód megváltoztatása gyógyszerek Treatment of mixed hyperlipidemia The management of the patient with mixed hyperlipidemia starts with TLC and progresses to LDL-C reduction to the LDL-C goal. If patients require additional treatment to achieve their secondary treatment goal defined by non-HDL-C, several approaches can be chosen. Statin therapy (or other LDL-C–lowering regimens) may be intensified, or triglyceride-lowering drugs may be added to the regimen. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Lépés 1 Elérni az LDL-C célértéket Elérni a nem-HDL-C célértéket tovább csökkenteni az LDL-C-t vagy kiegészíteni fibráttal, niacinnal vagy halolajjal Lépés 2 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
 may be intensified, or triglyceride-lowering drugs may be added to the regimen. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Lépés. 1. Elérni az LDL-C célértéket. Elérni a nem-HDL-C célértéket tovább csökkenteni az LDL-C-t vagy. kiegészíteni fibráttal, niacinnal vagy halolajjal. Lépés. 2. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:")
25
EUROAPIRE felmérések Gyógyszerhasználat: Sztatinok
S2 vs. S1 : P<0.0001 S3 vs. S2 : P<0.0001 S3 vs. S1 : P<0.0001 EUROASPIRE I ( ) EUROASPIRE II ( ) EUROASPIRE III ( )
 EUROASPIRE II ( ) EUROASPIRE III ( )")
26
Koleszterin kezelés: sztatinok
HMG-CoA reductáz gátlás (a koleszterin szintézis enzime) az LDL-C csökkentése 25 –60 %-kal, TG csökkentés HDL-C szint emelése Sztatin monoterápiával sok betegben nem lehet mindig elérni a terépiás célértéket A sztatinra adott terápiás válasz betegenként változik (interindividuális variabilitás) Mellékhatások korlátozhatják a használatot: Hepatotoxicitás (abnormális májfunkciós tesztek) Myopathia Slide 7 Statins provide powerful lipid-lowering efficacy by inhibiting HMG-CoA reductase, the rate-limiting enzyme for synthesis of cholesterol in the liver. The reduced hepatic cholesterol synthesis also upregulates LDL receptors and increases clearance of LDL from plasma. In clinical trials, statins decreased LDL-C by 25 to 60% and also reduced plasma levels of very-low-density lipoprotein (VLDL).3 Statins also decreased triglyceride levels in patients with hypertriglyceridemia, and increased HDL-C.21 Many patients receiving statins as monotherapy may fail to achieve and maintain the target goals at initial doses.22 Variations in response to statins between individuals exist.23 The use of statins also may be limited by adverse events, including hepatotoxicity (abnormalities on liver function tests), myopathy, and, in rare cases, rhabdomyolysis.21 Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998: ; Illingworth DR Med Clin North Am 2000;84:23-42; Andrews TC et al Am J Med 2001;111: ; Thompson GR et al Eur Heart J 2002;23:
 az LDL-C csökkentése 25 –60 %-kal, TG csökkentés. HDL-C szint emelése. Sztatin monoterápiával sok betegben nem lehet mindig elérni a terépiás célértéket. A sztatinra adott terápiás válasz betegenként változik (interindividuális variabilitás) Mellékhatások korlátozhatják a használatot: Hepatotoxicitás (abnormális májfunkciós tesztek) Myopathia. Slide 7. Statins provide powerful lipid-lowering efficacy by inhibiting HMG-CoA reductase, the rate-limiting enzyme for synthesis of cholesterol in the liver. The reduced hepatic cholesterol synthesis also upregulates LDL receptors and increases clearance of LDL from plasma. In clinical trials, statins decreased LDL-C by 25 to 60% and also reduced plasma levels of very-low-density lipoprotein (VLDL).3 Statins also decreased triglyceride levels in patients with hypertriglyceridemia, and increased HDL-C.21. Many patients receiving statins as monotherapy may fail to achieve and maintain the target goals at initial doses.22 Variations in response to statins between individuals exist.23 The use of statins also may be limited by adverse events, including hepatotoxicity (abnormalities on liver function tests), myopathy, and, in rare cases, rhabdomyolysis.21. Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998: ; Illingworth DR Med Clin North Am 2000;84:23-42; Andrews TC et al Am J Med 2001;111: ; Thompson GR et al Eur Heart J 2002;23:")
27
Koleszterin kezelés: egyéb szerek
Epesavkötő gyanták, ioncserélő gyanták az enterohepatikus epesav körforgás megszakítása LDL-C 20–30%-kal , VLDL-C , HDL-C , TG Niacin, nikotinsavamid A lipoprotein elválasztást gátolja LDL-C 15–25 %-kal , VLDL-C 25–35%-kal , HDL-C Fibrátok lipoprotein lipolysis indukálják, LDL-C lebontás , HDL termelés , koleszterin transzport megfordítása TG 25–40 % -kal , HDL-C , LDL-C or Slide 8 In addition to statins, three other cholesterol-lowering therapies are commonly used: bile acid–binding resins, nicotinic acid (niacin), and fibrates. Bile acid–binding resins interrupt the enterohepatic circulation of bile acids, increasing the synthesis of new bile acids and the expression of LDL receptors. They also decrease the synthesis of VLDL and LDL, reducing LDL-C by 20 to 30% and raising HDL-C and triglyceride levels.3 The mechanism by which niacin lowers cholesterol levels is not completely understood, but niacin appears to inhibit the secretion of apoB100-containing lipoproteins from the liver and may decrease LDL and VLDL synthesis. Nicotinic acid decreases triglycerides by 25 to 85%, VLDL-C by 25 to 35%, and LDL-C by 15 to 25%; HDL-C levels may be increased.3 Fibric acid derivatives, or fibrates, activate specific members of the nuclear hormone receptor family called peroxisome proliferator activator receptors (PPARs)21 and modulate lipoproteins through five major mechanisms: (1) induction of lipoprotein lipolysis; (2) reduction of hepatic triglyceride production; (3) increased HDL production and stimulation of reverse cholesterol transport; (4) reduced neutral lipid exchange; and (5) increased removal of LDL particles.24 Treatment with fibrates decreases triglycerides by 25 to 40% and increases HDL.3 VLDL-C = very-low-density lipoprotein cholesterol; HDL-C = high-density lipoprotein cholesterol; TG = triglycerides Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998: ; Illingworth DR Med Clin North Am 2000;84:23-42;Staels B et al Circulation 1998;98:
, and fibrates. Bile acid–binding resins interrupt the enterohepatic circulation of bile acids, increasing the synthesis of new bile acids and the expression of LDL receptors. They also decrease the synthesis of VLDL and LDL, reducing LDL-C by 20 to 30% and raising HDL-C and triglyceride levels.3. The mechanism by which niacin lowers cholesterol levels is not completely understood, but niacin appears to inhibit the secretion of apoB100-containing lipoproteins from the liver and may decrease LDL and VLDL synthesis. Nicotinic acid decreases triglycerides by 25 to 85%, VLDL-C by 25 to 35%, and LDL-C by 15 to 25%; HDL-C levels may be increased.3. Fibric acid derivatives, or fibrates, activate specific members of the nuclear hormone receptor family called peroxisome proliferator activator receptors (PPARs)21 and modulate lipoproteins through five major mechanisms: (1) induction of lipoprotein lipolysis; (2) reduction of hepatic triglyceride production; (3) increased HDL production and stimulation of reverse cholesterol transport; (4) reduced neutral lipid exchange; and (5) increased removal of LDL particles.24 Treatment with fibrates decreases triglycerides by 25 to 40% and increases HDL.3. VLDL-C = very-low-density lipoprotein cholesterol; HDL-C = high-density lipoprotein cholesterol; TG = triglycerides. Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998: ; Illingworth DR Med Clin North Am 2000;84:23-42;Staels B et al Circulation 1998;98:")
28
Sztatinok „extra-lipid” hatásai, melyek befolyásolják az atherosclerosist
Az endotél funkció befolyásolása Antioxidáns hatás Gyulladáscsökkentő hatás Antiproliferatív hatás Antitrombogén hatás

29
KVB rizikócsökkentés sztatin terápiával
Relativ Rizikó Redukció (%) Végpont +20 –5 –10 –15 –20 –25 –30 –35 –40 –45 –50 Koronária esemény Koronária halál Kardiovaszkuláris halál Nem kardiovaszk. esemény Össz mortalitás Stroke Claudicatio intermittens Angina CHD risk reduction with statin therapy Practically every clinical manifestation of atherosclerosis has been shown to be reduced by statin therapy, including fatal and nonfatal myocardial infarction, sudden CHD death, episodes of unstable angina, revascularization procedures including percutaneous transluminal coronary angioplasty (PTCA) and coronary artery bypass grafting (CABG), stroke, symptoms of peripheral arterial disease, and total mortality. Importantly, statin therapy has not been associated with an increase in noncardiovascular events. These data demonstrate that statins improve the quality of life (by reducing nonfatal events) and also lengthen life (by reducing total mortality). References: LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: a meta-analysis of randomized controlled trials. JAMA 1999;282: Crouse JR III, Byington RP, Hoen HM, Furberg CD. Reductase inhibitor monotherapy and stroke prevention. Arch Intern Med 1997;157: Pedersen TR, Kjekshus J, Pyorala K, Olsson AG, Cook TJ, Musliner TA, Tobert JA, Haghfelt T. Effect of simvastatin on ischemic signs and symptoms in the Scandinavian Simvastatin Survival Study (4S). Am J Cardiol 1998;81: La Rosa JC et al. JAMA 1999;282: | Crouse JR III et al. Arch Intern Med 1997;157: | Pedersen TR et al. Am J Cardiol 1998;81:
 Végpont –5. –10. –15. –20. –25. –30. –35. –40. –45. –50. Koronária esemény. Koronária halál. Kardiovaszkuláris halál. Nem kardiovaszk. esemény. Össz mortalitás. Stroke. Claudicatio intermittens. Angina. CHD risk reduction with statin therapy. Practically every clinical manifestation of atherosclerosis has been shown to be reduced by statin therapy, including fatal and nonfatal myocardial infarction, sudden CHD death, episodes of unstable angina, revascularization procedures including percutaneous transluminal coronary angioplasty (PTCA) and coronary artery bypass grafting (CABG), stroke, symptoms of peripheral arterial disease, and total mortality. Importantly, statin therapy has not been associated with an increase in noncardiovascular events. These data demonstrate that statins improve the quality of life (by reducing nonfatal events) and also lengthen life (by reducing total mortality). References: LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: a meta-analysis of randomized controlled trials. JAMA 1999;282: Crouse JR III, Byington RP, Hoen HM, Furberg CD. Reductase inhibitor monotherapy and stroke prevention. Arch Intern Med 1997;157: Pedersen TR, Kjekshus J, Pyorala K, Olsson AG, Cook TJ, Musliner TA, Tobert JA, Haghfelt T. Effect of simvastatin on ischemic signs and symptoms in the Scandinavian Simvastatin Survival Study (4S). Am J Cardiol 1998;81: La Rosa JC et al. JAMA 1999;282: | Crouse JR III et al. Arch Intern. Med 1997;157: | Pedersen TR et al. Am J Cardiol 1998;81:")
30
Sztatinok mellékhatásai
Általános mellékhatások - fejfájás – myalgia – fáradtság - GI* intolerancia – influenza-szerű tünetek Májenzim emelkedés Dózisfüggő, a betegek 0,5-2,5 %-ban fordul elő Súlyos májkárosodás igen ritka Teendő: sztatin dózis csökkentés vagy a kezelés abbahagyása; az enzimek rendeződnek Myopathia A betegek 0,2-0,4%-ban fordul elő Rhabdomyolysis igen ritka Csökkenthető Vesekárosodás esetén óvatos kezelés A legalacsonyabb hatásos dózist kell adni Sztatin – fibrát kombináció csak szükséges esetben, igen óvatosan Kerülni a gyógyszerinterakciókat A tünetek szoros monitorozása Izomkárosodás tüneteinek jelentkezésekor a sztatin kezelést azonnal abba kell hagyni Statin adverse events Statins are very safe. 95% of patients can tolerate them; 5% cannot. Common side effects include headache, upset stomach, fatigue, flu-like symptoms, and myalgia (without changes in creatine kinase [CK]). One or both liver transaminases may be elevated to >3 times the upper limit of normal on two consecutive occasions in 0.5% (with starting doses) to as high as 2.5% (with high doses) of patients in a dose-dependent manner. Whether statin-induced elevations in liver enzymes constitute true hepatotoxicity has not been determined. Cases of serious liver dysfunction or failure are exceedingly rare and not clearly related to statin therapy. Enzymes will frequently return to normal by reducing doses or even with continuation of therapy. If an elevation persists, discontinuation of therapy for a short period until levels return to normal is advised. Statin therapy may then be reinitiated. Myopathy defined as muscle symptoms (muscle weakness, aches, or soreness) plus CK >10 times the upper limit of normal is seen in 2–4 patients per In 77,000 patient-years of use in the landmark clinical trials, 8 cases of myopathy were reported. Very rare cases of rhabdomyolysis, myoglobinuria, acute renal necrosis, and death have been reported. The incidence of myopathy appears related to the systemic blood concentration of the statin. Myopathy is most likely to occur with higher doses, in patients with renal impairment, when a statin is combined with a fibrate, when a drug interfering with the metabolism of the statin is given concurrently (e.g., macrolide antibiotics, certain antifungal medications, gemfibrozil, cyclosporine), and in elderly women. All patients started on statins should be instructed to report immediately muscle symptoms or brown urine and to have CK measured. If myopathy is present or strongly suspected, the statin should be discontinued immediately. * GI gasztrointesztinális
. One or both liver transaminases may be elevated to >3 times the upper limit of normal on two consecutive occasions in 0.5% (with starting doses) to as high as 2.5% (with high doses) of patients in a dose-dependent manner. Whether statin-induced elevations in liver enzymes constitute true hepatotoxicity has not been determined. Cases of serious liver dysfunction or failure are exceedingly rare and not clearly related to statin therapy. Enzymes will frequently return to normal by reducing doses or even with continuation of therapy. If an elevation persists, discontinuation of therapy for a short period until levels return to normal is advised. Statin therapy may then be reinitiated. Myopathy defined as muscle symptoms (muscle weakness, aches, or soreness) plus CK >10 times the upper limit of normal is seen in 2–4 patients per In 77,000 patient-years of use in the landmark clinical trials, 8 cases of myopathy were reported. Very rare cases of rhabdomyolysis, myoglobinuria, acute renal necrosis, and death have been reported. The incidence of myopathy appears related to the systemic blood concentration of the statin. Myopathy is most likely to occur with higher doses, in patients with renal impairment, when a statin is combined with a fibrate, when a drug interfering with the metabolism of the statin is given concurrently (e.g., macrolide antibiotics, certain antifungal medications, gemfibrozil, cyclosporine), and in elderly women. All patients started on statins should be instructed to report immediately muscle symptoms or brown urine and to have CK measured. If myopathy is present or strongly suspected, the statin should be discontinued immediately. * GI gasztrointesztinális.")
31
A sztatin hatás időbeli lefolyása
Vulnerábilis plakk stabilizálódik LDL-C csökken gyulladás csökken Endotél funkció javul Isémiás epizód csökken Kardiális események csökkennek* Potential time course of statin effects CHD risk reduction with a statin appears to occur as a result of several related changes, including restoration of endothelial function, reduction in inflammation, and stabilization of vulnerable plaque. The time course for these antiatherosclerotic effects of statins ranges from days to years. Within weeks to months after beginning statin therapy, endothelial function of coronary arteries is restored. Concurrent with this or following by just a few months is a reduction in inflammatory markers, such as high-sensitivity C-reactive protein. These effects appear to coincide with the reduction in ischemic events demonstrated after about 18 months of statin therapy. After several years of therapy (i.e., 1.5–2.5 years), fatal and nonfatal myocardial infarction rates begin to decline in statin-treated patients, and after 5 years of therapy, significant reductions have been documented. These changes coincide somewhat with stabilization of vulnerable atherosclerotic plaque during which the lipid-rich core of plaque is replaced with connective tissue and matrix. Napok Évek * Időbeli alakulás kimutatható
, fatal and nonfatal myocardial infarction rates begin to decline in statin-treated patients, and after 5 years of therapy, significant reductions have been documented. These changes coincide somewhat with stabilization of vulnerable atherosclerotic plaque during which the lipid-rich core of plaque is replaced with connective tissue and matrix. Napok. Évek. * Időbeli alakulás kimutatható.")
32
Hogyan lehet minimalizálni az izomtoxicitást sztatin -fibrát kombinált terápia során?
Ha a terápiás cél a nem-HDL-C csökkentése, sztatin monoterápia javasolt Alacsony sztatin és fibrát adagok A fibrátot reggel / délelőtt, a sztatint délután / este vegye be a beteg Vesekárosodásban kerülni kell a kombinált kezelést Egyéb gyógyszerinterakció se legyen Meg kell tanítani a pácienst az izomproblémák felismerésére A kezelést abba kell hagyni az izomkárosodás tüneteinek jelentkezésekor vagy ha a szérum kreatinin szint 10x nő Steps to minimize the risk of muscle toxicity with fibrate–statin combination therapy The greatest issue with the use of a fibrate and statin in combination is the increased risk of causing myopathy and rhabdomyolysis. This risk is enhanced with high statin doses, in the presence of renal insufficiency, in older patients, and whenever drugs that may interfere with statin metabolism are given concurrently. To minimize the muscle side effects when combining any of these drugs with a statin, the following suggestions are made. Try to achieve LDL-C and non-HDL-C treatment goals with a statin alone. If adding a triglyceride-lowering drug to the statin, give preference to fish oils or niacin, as the risk of myopathy appears low. If a fibrate is to be added, fenofibrate is preferred over gemfibrozil, since there may be a lower risk of myopathy. Use the lowest effective dose of both the statin and fibrate to achieve treatment goals (e.g., starting dose of a statin with 63–126 mg of fenofibrate). Dose the fibrate in the morning and the statin in the evening (note that this suggestion is based on theoretical considerations and not on any evidence that this recommendation will reduce the incidence of muscle toxicity). Avoid (or cautiously use) statins in patients who have compromised renal function (as is often found in elderly patients) or hepatic function (including alcoholics). Assure that no other drugs are or will be used concurrently that could interfere with the metabolism of the statin. Obtain a baseline CK level and repeat it during the course of therapy if the patient reports muscle symptoms. Teach the patient to recognize and report muscle weakness, tenderness, or pain and be prepared to evaluate patients who experience these symptoms. Discontinue therapy if muscle symptoms are present and a CK is >10 times the upper limit of normal.
. Dose the fibrate in the morning and the statin in the evening (note that this suggestion is based on theoretical considerations and not on any evidence that this recommendation will reduce the incidence of muscle toxicity). Avoid (or cautiously use) statins in patients who have compromised renal function (as is often found in elderly patients) or hepatic function (including alcoholics). Assure that no other drugs are or will be used concurrently that could interfere with the metabolism of the statin. Obtain a baseline CK level and repeat it during the course of therapy if the patient reports muscle symptoms. Teach the patient to recognize and report muscle weakness, tenderness, or pain and be prepared to evaluate patients who experience these symptoms. Discontinue therapy if muscle symptoms are present and a CK is >10 times the upper limit of normal.")
33
Fibrátok Javallat: Diéta mellé adjuváns kezelés Hypertriglyceridemia
Kombinált hyperlipidemia with alacsony HDL-C szinttel Hatásmechanizmus: Növelik a periférián a lipolysist és csökkentik a májban a TG termelést Hatékonyság : TG 25–50%- kal csökken LDL-C csökken/változatlan/nő hypertriglyceridemia-ban nő a HDL-C + 15–25%-kal Mellékhatás : GI panasz (8%), epekő, myositis, májfunkciós eltérések Ellenjavallat : Máj- vagy vesekárosodás meglévő epehólyag betegség Fibric acid derivatives The final group of triglyceride-lowering drugs that may be useful in reaching non-HDL-C goals is the fibrates. The mechanism of action of fibrates is very complex and not entirely understood. Their principal effect appears to be mediated through nuclear transcription factor peroxisome proliferator-activated receptor (PPAR-) in liver, adipose, and other tissues. Their agonist effect on these receptors down-regulates the apo C-III gene and up-regulates genes for apo A-I, fatty acid transport protein, fatty acid oxidation, and possibly lipoprotein lipase. The effects on lipoprotein lipase and apo C-III (which inhibits lipoprotein lipase) enhance the catabolism of triglyceride-rich lipoproteins, whereas increased fatty acid oxidation reduces formation of VLDL triglycerides. Increased synthesis of apo A-I tends to raise HDL-C levels. The prominent effect of the fibrates is to reduce elevated triglyceride by 25–50% and secondarily to raise HDL-C by 15–25%. Fibrates are generally well tolerated in most patients. GI complaints are the most common side effects. All drugs in this class appear to increase the lithogenicity of bile and increase the likelihood of cholesterol gallstones. Additionally, the fibrates are highly bound to serum albumin and may displace warfarin, increasing its anticoagulant effects. Since fibrates are excreted primarily by the kidneys, caution should be observed in patients with renal failure. Myopathy has been observed particularly when combined with a statin. More comment will be given to this issue in slide 30. References: Frick MH, Elo O, Haapa K, Heinonen OP, Heinsalmi P, Helo P, Huttunen JK, Kaitaniemi P, Koskinen P, Manninen V, Mäenpää H, Mälkönen M, Mänttäri M, Norola S, Pasternack A, Pikkarainen J, Romo M, Sjöblom T, Nikkilä EA. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med 1987;317: Frick MH, Syvänne M, Nieminen MS, Kauma H, Majahalme S, Virtanen V, Kesäniemi YA, Pasternack A, Taskinen M-R, for the Lopid Coronary Angiography Trial (LOCAT) Study Group. Prevention of the angiographic progression of coronary and vein-graft atherosclerosis by gemfibrozil after coronary bypass surgery in men with low levels of HDL cholesterol. Circulation 1997;96: Ericsson C-G, Hamsten A, Nilsson J, Grip L, Svane B, de Faire U. Angiographic assessment of effects of bezafibrate on progression of coronary artery disease in young male postinfarction patients. Lancet 1996;347: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: The BIP Study Group. Secondary prevention by raising HDL cholesterol and reducing triglycerides in patients with coronary artery disease: the Bezafibrate Infarction Prevention (BIP) Study. Circulation 2000;102:21-27.
, epekő, myositis, májfunkciós eltérések. Ellenjavallat : Máj- vagy vesekárosodás meglévő epehólyag betegség. Fibric acid derivatives. The final group of triglyceride-lowering drugs that may be useful in reaching non-HDL-C goals is the fibrates. The mechanism of action of fibrates is very complex and not entirely understood. Their principal effect appears to be mediated through nuclear transcription factor peroxisome proliferator-activated receptor (PPAR-) in liver, adipose, and other tissues. Their agonist effect on these receptors down-regulates the apo C-III gene and up-regulates genes for apo A-I, fatty acid transport protein, fatty acid oxidation, and possibly lipoprotein lipase. The effects on lipoprotein lipase and apo C-III (which inhibits lipoprotein lipase) enhance the catabolism of triglyceride-rich lipoproteins, whereas increased fatty acid oxidation reduces formation of VLDL triglycerides. Increased synthesis of apo A-I tends to raise HDL-C levels. The prominent effect of the fibrates is to reduce elevated triglyceride by 25–50% and secondarily to raise HDL-C by 15–25%. Fibrates are generally well tolerated in most patients. GI complaints are the most common side effects. All drugs in this class appear to increase the lithogenicity of bile and increase the likelihood of cholesterol gallstones. Additionally, the fibrates are highly bound to serum albumin and may displace warfarin, increasing its anticoagulant effects. Since fibrates are excreted primarily by the kidneys, caution should be observed in patients with renal failure. Myopathy has been observed particularly when combined with a statin. More comment will be given to this issue in slide 30. References: Frick MH, Elo O, Haapa K, Heinonen OP, Heinsalmi P, Helo P, Huttunen JK, Kaitaniemi P, Koskinen P, Manninen V, Mäenpää H, Mälkönen M, Mänttäri M, Norola S, Pasternack A, Pikkarainen J, Romo M, Sjöblom T, Nikkilä EA. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med 1987;317: Frick MH, Syvänne M, Nieminen MS, Kauma H, Majahalme S, Virtanen V, Kesäniemi YA, Pasternack A, Taskinen M-R, for the Lopid Coronary Angiography Trial (LOCAT) Study Group. Prevention of the angiographic progression of coronary and vein-graft atherosclerosis by gemfibrozil after coronary bypass surgery in men with low levels of HDL cholesterol. Circulation 1997;96: Ericsson C-G, Hamsten A, Nilsson J, Grip L, Svane B, de Faire U. Angiographic assessment of effects of bezafibrate on progression of coronary artery disease in young male postinfarction patients. Lancet 1996;347: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: The BIP Study Group. Secondary prevention by raising HDL cholesterol and reducing triglycerides in patients with coronary artery disease: the Bezafibrate Infarction Prevention (BIP) Study. Circulation 2000;102:")
34
Hyperlipidemia kezelése
Életmódváltoztatás Izolált hypercholesterinemia (magas LDL-C, TG<5mmol) Kombinált dyslipidemia (magas LDL-C, High TG) Izolált Triglycerinemia (alacsony LDL-C, TG>5mmol) Monoterápia 1 sztatin sztatin fibrat niacin fibrat niacin 2 ezetimib gyanta Treatment of hyperlipidemia Statins have been and remain the drugs of first choice for lowering LDL-C. They lower LDL-C more effectively than other currently available agents, and they reduce CHD risk. Because of their LDL-C–lowering efficacy, they are able to achieve LDL-C treatment goals in the majority of patients, regardless of their risk category. In fact, the more potent the LDL-C–lowering efficacy of the statin, the greater the percentage of patients who will achieve their LDL-C goal. Statins are also remarkably safe as will be described below. About 5–10% of patients will not be able to tolerate a statin and so the only alternative agents for lowering LDL-C are a bile acid resin and niacin. These drugs are not as effective in lowering LDL-C and cause bothersome side effects which make patient compliance a problem. However, they are effective in reducing CHD risk and in the majority of patients can be successfully taken. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Kombinációs terápia (ha a mono nem elég) 2 S+fibrat S+ezetimib S+niacin egyéb (gyanták) 3 Ha a kombinációs kezelés ellenére sem éri el a páciens a célértéket LDL-aferesis
 Kombinált. dyslipidemia. (magas LDL-C, High TG) Izolált. Triglycerinemia. (alacsony LDL-C, TG>5mmol) Monoterápia. 1. sztatin. sztatin. fibrat. niacin. fibrat. niacin. 2. ezetimib. gyanta. Treatment of hyperlipidemia. Statins have been and remain the drugs of first choice for lowering LDL-C. They lower LDL-C more effectively than other currently available agents, and they reduce CHD risk. Because of their LDL-C–lowering efficacy, they are able to achieve LDL-C treatment goals in the majority of patients, regardless of their risk category. In fact, the more potent the LDL-C–lowering efficacy of the statin, the greater the percentage of patients who will achieve their LDL-C goal. Statins are also remarkably safe as will be described below. About 5–10% of patients will not be able to tolerate a statin and so the only alternative agents for lowering LDL-C are a bile acid resin and niacin. These drugs are not as effective in lowering LDL-C and cause bothersome side effects which make patient compliance a problem. However, they are effective in reducing CHD risk and in the majority of patients can be successfully taken. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Kombinációs terápia. (ha a mono nem elég) 2. S+fibrat. S+ezetimib. S+niacin. egyéb. (gyanták) 3. Ha a kombinációs kezelés ellenére sem éri el a páciens a célértéket. LDL-aferesis.")
35
Páciens tolerabilitás
Lipidcsökkentő gyógyszeres kezelés Terápia Össz C LDL HDL TG Páciens tolerabilitás Sztatinok* ¯ % ¯ % 4-12% ¯ % Jó Ezetimib ¯ 13% ¯ 18% 1% ¯ 9% Epesav-kötők ¯ % ¯ % 3% - vagy Rossz Nikotinsav ¯ % % ¯ % Elviselhető - rossz Fibrátok ¯ 19% ¯ 4-21% % ¯ 30% Lipid-modifying therapies include HMG CoA reductase inhibitors (statins), fibrates, bile acid sequestrants (resins), nicotinic acid and its derivatives, and probucol. Statins are highly effective in lowering LDL-cholesterol and have a good tolerability profile.1-3 Data presented in this slide does not include rosuvastatin. Bile acid sequestrants are potent cholesterol-modifying agents. Adverse events such as gastrointestinal bloating, nausea and constipation limit compliance to the bile acid sequestrants.1,2 Nicotinic acid, a B-complex vitamin, is effective at reducing both LDL cholesterol and triglyceride concentrations, and increasing HDL cholesterol levels. To be effective, it must be given in pharmacologic doses. The value of nicotinic acid has been limited by the incidence of adverse events, which include flushing, skin problems, gastrointestinal distress, liver toxicity, hyperglycaemia and hyperuricemia.1,2 Fibrates are effective triglyceride-lowering and HDL-raising drugs. However, in the majority of patients they are only moderately successful in reducing LDL-cholesterol.1,2 Probucol is not available in most countries. It has only a modest LDL-cholesterol-lowering effect, and there is no evidence that it reduces CHD risk and there are limited long-term tolerability data.1,2 Ezetimibe is the first of a novel class of selective cholesterol-absorption inhibitors. Ezetimibe may be useful in patients who are intolerant to other lipid-modifying therapies, and in combination with a statin in patients who are intolerant to large doses of statins or need further reductions in LDL cholesterol despite maximum doses of a statin.4 References 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391. 2. National Cholesterol Education Program. Circulation 1994;98(3):1333–1445. 3. Knopp RH. N Engl J Med 1999;341:498–511. 4. Gupta EK, Ito MK. Heart Dis 2002;4:399–409. HDL-C=High-density lipoprotein cholesterol, LDL-C=Low-density lipoprotein cholesterol, TC=Total cholesterol, TG=Triglycerides *Mindegyik hatóanyagból 40 mg/nap, kivéve rosuvastatin.
, fibrates, bile acid sequestrants (resins), nicotinic acid and its derivatives, and probucol. Statins are highly effective in lowering LDL-cholesterol and have a good tolerability profile.1-3 Data presented in this slide does not include rosuvastatin. Bile acid sequestrants are potent cholesterol-modifying agents. Adverse events such as gastrointestinal bloating, nausea and constipation limit compliance to the bile acid sequestrants.1,2. Nicotinic acid, a B-complex vitamin, is effective at reducing both LDL cholesterol and triglyceride concentrations, and increasing HDL cholesterol levels. To be effective, it must be given in pharmacologic doses. The value of nicotinic acid has been limited by the incidence of adverse events, which include flushing, skin problems, gastrointestinal distress, liver toxicity, hyperglycaemia and hyperuricemia.1,2. Fibrates are effective triglyceride-lowering and HDL-raising drugs. However, in the majority of patients they are only moderately successful in reducing LDL-cholesterol.1,2. Probucol is not available in most countries. It has only a modest LDL-cholesterol-lowering effect, and there is no evidence that it reduces CHD risk and there are limited long-term tolerability data.1,2. Ezetimibe is the first of a novel class of selective cholesterol-absorption inhibitors. Ezetimibe may be useful in patients who are intolerant to other lipid-modifying therapies, and in combination with a statin in patients who are intolerant to large doses of statins or need further reductions in LDL cholesterol despite maximum doses of a statin.4. References. 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379– National Cholesterol Education Program. Circulation 1994;98(3):1333– Knopp RH. N Engl J Med 1999;341:498– Gupta EK, Ito MK. Heart Dis 2002;4:399–409. HDL-C=High-density lipoprotein cholesterol, LDL-C=Low-density lipoprotein cholesterol, TC=Total cholesterol, TG=Triglycerides. *Mindegyik hatóanyagból 40 mg/nap, kivéve rosuvastatin.")
36
C reaktív protein (CRP) és a kardiovaszkuláris rizikó
CRP a gyulladás kiváló markere CRP emelkedése arányos a KVB és mortalitás rizikójának növekedésével Bizonyított kezelések (ASA, clopidogrel, sztatin) Hatékonyabbak emelkedett CRP esetén Némelyik csökkenti a CRP szintet (sztatinok) PROVE IT–TIMI 22 és a REVERSAL vizsgálat bizonyította, hogy a gyulladáscsökkentés mérsékli az atheroscleroticus folyamat ütemét és javítja a kimenetelt ? További vizsgálat szükséges: CRP csökkentés vs. standard kardiológiai rehabilitáció / rizikófaktor csökkentés CRP and CV risk Thus, we have seen that CRP is well known as a marker of inflammation, and elevated CRP correlates with an increased risk for cardiac events and mortality. Many proven therapies such as aspirin, clopidogrel, and statins have a greater benefit on preventing cardiac events among patients with an elevated CRP. In some cases, these agents also reduce CRP, such as the statins (but not aspirin). Now, evidence from PROVE IT–TIMI 22 and REVERSAL has shown that targeting CRP levels may be a means of reducing atherosclerosis and optimizing clinical outcomes. However, there is a need for additional data using different classes of drugs and/or CRP-based risk factor modification to bring full circle the notion that control of risk factors would be beneficial on CRP and on clinical outcomes. Thus, these are very promising times to look at CRP as a marker of overall vascular health that could be used to target our aggressiveness of medical therapy and lifestyle modification.
 Hatékonyabbak emelkedett CRP esetén. Némelyik csökkenti a CRP szintet (sztatinok) PROVE IT–TIMI 22 és a REVERSAL vizsgálat bizonyította, hogy a gyulladáscsökkentés mérsékli az atheroscleroticus folyamat ütemét és javítja a kimenetelt. További vizsgálat szükséges: CRP csökkentés vs. standard kardiológiai rehabilitáció / rizikófaktor csökkentés. CRP and CV risk. Thus, we have seen that CRP is well known as a marker of inflammation, and elevated CRP correlates with an increased risk for cardiac events and mortality. Many proven therapies such as aspirin, clopidogrel, and statins have a greater benefit on preventing cardiac events among patients with an elevated CRP. In some cases, these agents also reduce CRP, such as the statins (but not aspirin). Now, evidence from PROVE IT–TIMI 22 and REVERSAL has shown that targeting CRP levels may be a means of reducing atherosclerosis and optimizing clinical outcomes. However, there is a need for additional data using different classes of drugs and/or CRP-based risk factor modification to bring full circle the notion that control of risk factors would be beneficial on CRP and on clinical outcomes. Thus, these are very promising times to look at CRP as a marker of overall vascular health that could be used to target our aggressiveness of medical therapy and lifestyle modification.")
37
Az atherosclerosis gyakori az újonnan diagnosztizált diabeteses betegek körében
A KVB gyakori betegség a diabeteses betegek körében, illetve halálokként is gyakori Az újonnan felfedezett diabeteses betegek >50%-ánál a KVB jelenléte bizonyítható Az atherosclerosis a vezető halálokok egyike diabeteses betegeknél 75% koronária atherosclerosis 25% cerebralis vagy perifériás érbetegség miatt A diabeteses betegek körében előforduló hospitalizáció >75% atheroscleroticus okra vezethető vissza The risk for CHD in individuals with diabetes is high. Cardiovascular diseases, including CHD, stroke, and peripheral vascular disease, are common causes of morbidity and mortality among people with diabetes, and >50% of patients with newly diagnosed type 2 diabetes show evidence of cardiovascular disease.5,6 Among patients with diabetes, 75% of deaths attributed to atherosclerosis are due to coronary atherosclerosis and 25% are the result of either cerebral or peripheral vascular disease.6 Epidemiologic data also indicate that >75% of all hospitalizations for individuals with diabetes are related to atherosclerotic disease. The prognosis for patients with CHD is worse in individuals who also have diabetes than for those who do not.7-9 Amos AF et al Diab Med 1997;14:S7-S85; Hill Golden S Adv Stud Med 2002;2: ; Haffner SM et al N Engl J Med 1998;339: ; Sprafka JM et al Diabetes Care 1991;14:

38
KV mortalitás per 10,000 betegév össz koleszterin (mmol/l)
Az alacsony koleszterinszinttel rendelkező diabéteszes beteg kardiovaszkuláris kockázata magasabb, mint a magas koleszterinszinttel rendelkező, de nem diabéteszes betegeké! 160 Diabétesz Nincs diabétesz 140 120 100 KV mortalitás per 10,000 betegév 80 60 40 20 People with diabetes and low cholesterol were at greater risk of cardiovascular mortality than people without diabetes and high cholesterol, as seen in MRFIT. Assessment of risk for cardiovascular death as a function of serum total cholesterol (TC) for men with and without diabetes in MRFIT indicated considerable excess risk for men with diabetes at each cholesterol level. Among men with serum TC <180 mg/dl, the death rate was per 10,000 person-years for men with diabetes compared with per 10,000 person-years for men without diabetes. Among men with TC 280 mg/dl, the respective values were and The relative risk for cardiovascular death among men with diabetes versus men without diabetes ranged from 2.83 to 4.46 across the evaluated levels of TC.14 Most striking, cardiovascular mortality is higher in patients with diabetes and low TC than in nondiabetic patients with high TC (dashed line). <4,7 4,7–5,1 5,2–5,7 5,8–6,2 6,3–6,7 6,8–7,2 >7,3 össz koleszterin (mmol/l) KV = kardiovaszkuláris Stamler J et al Diabetes Care 1993;16:
 for men with and without diabetes in MRFIT indicated considerable excess risk for men with diabetes at each cholesterol level. Among men with serum TC <180 mg/dl, the death rate was per 10,000 person-years for men with diabetes compared with per 10,000 person-years for men without diabetes. Among men with TC 280 mg/dl, the respective values were and The relative risk for cardiovascular death among men with diabetes versus men without diabetes ranged from 2.83 to 4.46 across the evaluated levels of TC.14 Most striking, cardiovascular mortality is higher in patients with diabetes and low TC than in nondiabetic patients with high TC (dashed line). <4,7. 4,7–5,1. 5,2–5,7. 5,8–6,2. 6,3–6,7. 6,8–7,2. >7,3. össz koleszterin (mmol/l) KV = kardiovaszkuláris. Stamler J et al Diabetes Care 1993;16:")