Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Perifériás érbetegségek
atherosclerosis

2
A kardiovaszkuláris halálozás Európában
Férfi (%) Nő (%) 44 38 45 31 38 34 37 29 32 29 40 39 Férfi (%) Nő (%) AHA Heart and Stroke Statistical Update* KSH 1999
 Nő (%) Férfi (%) Nő (%) AHA Heart and Stroke Statistical Update* KSH")
3
Az atherosclerosis fő előfordulási helyei
Cerebrovascularis szűkület Koszorúér szűkület Vese artéria szűkület Visceralis artériák szűkülete Perifériás artériák szűkülete Claudicatio intermittens A végtag kritikus ischaemiaja Major Manifestations of Atherothrombosis Vascular disease leading to atherothrombosis, is the result of a generalized process that affects multiple vascular beds, including the cerebral, coronary, and peripheral arteries. Coexistence of vascular disease in multiple beds increases the risk for developing ischemic events such as MI and stroke.1 Atherothrombosis in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours, but the majority resolve within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 8-12% during the first week following a TIA and 11-15% at one month. 2 Atherothrombosis in coronary arteries produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI). Cardiovascular disease is the single largest cause of death in the United States and Europe.3 Atherothrombosis in peripheral vessels, known as peripheral arterial disease (PAD), can produce a variety of symptoms ranging from intermittent claudication to pain at rest.4 Patients with the most serious PAD have critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis. 4 PAD is a strong marker for cardiovascular disease. Over a 10-year period, PAD increases risk for death due to cardiovascular disease approximately 6-fold.5 Note: Clopidogrel is not indicated for all the conditions listed on this slide. References: Aronow WS, Ahn C. Prevalence of coexistence of coronary artery disease, peripheral arterial disease, and atherothrombotic brain infarction in men and women 62 years of age. Am J Cardiol 1994; 74: Coull AJ, Lovett JK, Rothwell PM . Population based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organisation of services. BMJ 2004; 328 (7435): 32. American Heart Association Heart and Stroke Statistical Update. Weitz JI, Byrne J, Clagett GP et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation 1996; 94: Criqui MH, Langer RD, Fronek A et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992; 326:
 or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours, but the majority resolve within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 8-12% during the first week following a TIA and 11-15% at one month. 2. Atherothrombosis in coronary arteries produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI). Cardiovascular disease is the single largest cause of death in the United States and Europe.3. Atherothrombosis in peripheral vessels, known as peripheral arterial disease (PAD), can produce a variety of symptoms ranging from intermittent claudication to pain at rest.4. Patients with the most serious PAD have critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis. 4 PAD is a strong marker for cardiovascular disease. Over a 10-year period, PAD increases risk for death due to cardiovascular disease approximately 6-fold.5. Note: Clopidogrel is not indicated for all the conditions listed on this slide. References: Aronow WS, Ahn C. Prevalence of coexistence of coronary artery disease, peripheral arterial disease, and atherothrombotic brain infarction in men and women 62 years of age. Am J Cardiol 1994; 74: Coull AJ, Lovett JK, Rothwell PM . Population based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organisation of services. BMJ 2004; 328 (7435): 32. American Heart Association Heart and Stroke Statistical Update. Weitz JI, Byrne J, Clagett GP et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation 1996; 94: Criqui MH, Langer RD, Fronek A et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992; 326:")
4
Az atherothrombózis klinikai manifesztációi
Agyi Ischaemiás stroke TIA Szív Myocardialis infarctus Angina pectoris (stabil, instabil) Peripheriás Arteriás Megbetegedés Kritikus végtagi ischaemia, claudicatio Visceralis artériák keringési elégtelensége Intestinalis ischaemia, puffadás, hasmenés, fogyás, akut mesenterialis thrombosis Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1 Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2 Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: 2 American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: 3 Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:
 Peripheriás Arteriás Megbetegedés. Kritikus végtagi ischaemia, claudicatio. Visceralis artériák keringési elégtelensége. Intestinalis ischaemia, puffadás, hasmenés, fogyás, akut mesenterialis thrombosis. Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1. Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2. Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References. 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: identifier= Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:")
5
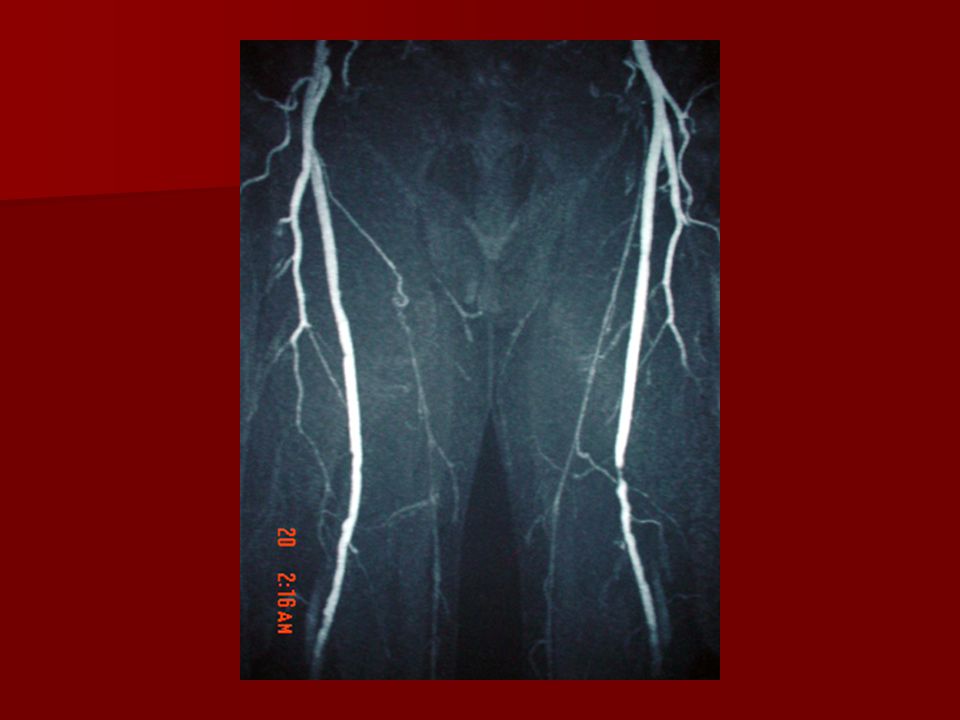
Az atherothrombózis vizsgálata
Anamnézis: Fájdalom (nyugalmi), claudicatio intermittens, dysbasiás távolság, gangraena, impotentia Fizikális vizsgálat: Perifériás artériák vizsgálata: inspekció, palpatio, auscultatio, Art. carotis,- brachialis,- radialis, -femoralis,- poplitea, -dorsalis pedis, - tibialis posterior Vénák vizsgálata: varicositas, körfogat Boka-brachialis index: 0,8 alatti érték claudicatiot jelez Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1 Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2 Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: 2 American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: 3 Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:
, claudicatio intermittens, dysbasiás távolság, gangraena, impotentia. Fizikális vizsgálat: Perifériás artériák vizsgálata: inspekció, palpatio, auscultatio, Art. carotis,- brachialis,- radialis, -femoralis,- poplitea, -dorsalis pedis, - tibialis posterior. Vénák vizsgálata: varicositas, körfogat. Boka-brachialis index: 0,8 alatti érték claudicatiot jelez. Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1. Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2. Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References. 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: identifier= Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:")
6
Az atherothrombózis vizsgálata
Duplex UH, MRI Angiographia: amennyiben percutan vagy nyitott műtét szóba jöhet Fokozott atherosclerosist jelez, CV rizikó nő Art renalis stenosis: renovascularis hypertonia (5%), duplex UH, veseszcintigráfia captoprillel, MRI Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1 Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2 Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: 2 American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: 3 Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:
, duplex UH, veseszcintigráfia captoprillel, MRI. Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1. Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2. Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References. 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: identifier= Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:")
9
A PAD előfordulása az életkorral nő
Rotterdam Study (ABI Test <0.9) San Diego Study (PAD by noninvasive tests)2 PAD betegek (%) Prevalence of PAD increases with age The prevalence of peripheral arterial disease (PAD) is age dependent. In the Rotterdam study (n=5,450), the prevalence of PAD based on the ankle-brachial index (ABI) increased from 9% of subjects 55 to 59 years of age to 57% of patients 85 to 89 years of age.1 Similarly, the prevalence of PAD increased from 2.5% in subjects 40 to 59 years of age to 18.8% in subjects 70 to 79 years of age in the San Diego population study (n=624). Prevalence was diagnosed using noninvasive tests of limb perfusion: segmental blood pressure, flow velocity, postocclusive reactive hyperemia and pulse reappearance half time.2 Discussion Points Based on the statistics from the Rotterdam study, in a practice of 2,000 patients with about 300 patients over 85 it could be estimated that approximately 170 patients would be diagnosed with PAD. Q. How does this correlate to the experience in your own practice; how many patients would you estimate have been diagnosed with PAD in your patient population and how many might there be of whom you are not aware? References: Meijer WT, Hoes AW, Rutgers D et al. Peripheral arterial disease in the elderly: the Rotterdam Study. Arterioscler Thromb Vasc Biol 1998; 18: Criqui MH, Fronek A, Barrett-Connor E et al. The prevalence of peripheral arterial disease in a defined population. Circulation 1985; 71: Figure adapted from Creager M, ed. Management of Peripheral Arterial Disease. Medical, Surgical and Interventional Aspects 1 Meijer WT et al. Arterioscler Thromb Vasc Biol 1998; 18: 2.Criqui MH et al. Circulation 1985; 71:
1 San Diego Study (PAD by noninvasive tests)2. PAD betegek (%) Prevalence of PAD increases with age. The prevalence of peripheral arterial disease (PAD) is age dependent. In the Rotterdam study (n=5,450), the prevalence of PAD based on the ankle-brachial index (ABI) increased from 9% of subjects 55 to 59 years of age to 57% of patients 85 to 89 years of age.1. Similarly, the prevalence of PAD increased from 2.5% in subjects 40 to 59 years of age to 18.8% in subjects 70 to 79 years of age in the San Diego population study (n=624). Prevalence was diagnosed using noninvasive tests of limb perfusion: segmental blood pressure, flow velocity, postocclusive reactive hyperemia and pulse reappearance half time.2. Discussion Points. Based on the statistics from the Rotterdam study, in a practice of 2,000 patients with about 300 patients over 85 it could be estimated that approximately 170 patients would be diagnosed with PAD. Q. How does this correlate to the experience in your own practice; how many patients would you estimate have been diagnosed with PAD in your patient population and how many might there be of whom you are not aware References: Meijer WT, Hoes AW, Rutgers D et al. Peripheral arterial disease in the elderly: the Rotterdam Study. Arterioscler Thromb Vasc Biol 1998; 18: Criqui MH, Fronek A, Barrett-Connor E et al. The prevalence of peripheral arterial disease in a defined population. Circulation 1985; 71: Figure adapted from Creager M, ed. Management of Peripheral Arterial Disease. Medical, Surgical and Interventional Aspects Meijer WT et al. Arterioscler Thromb Vasc Biol 1998; 18: Criqui MH et al. Circulation 1985; 71:")
10
Szoros korreláció található a boka-kar index értékének csökkenése és a kardiovaszkuláris rizikó között % 70 60 Összes halálozás Kardiovaszkuláris halálozás 50 40 30 There is a strong two-way association between decreased ABI and increased risk for cardiovascular death There is a clear association between the extent of PAD and the risk of myocardial infarction (MI) and stroke1. Reference: 1. Dormandy JA, Creager MA. Ankle: arm blood pressure index as a predictor of atherothrombotic events: evidence from CAPRIE. Cerebrovasc Dis 1999; 9(suppl 1): 14. 20 10 <0.60 (n=25) 0.60-<0.70 (n=21) 1.0-<1.10 (n=980) 0.70-<0.80 (n=40) 0.80-<0.90 (n=130) 0.90-<1.0 (n=195) Kiindulási boka-kar index *Az átlagos követési idő 8.3 év Resnick HE et al. Circulation 2004; 109:
 and stroke1. Reference: 1. Dormandy JA, Creager MA. Ankle: arm blood pressure index as a predictor of atherothrombotic events: evidence from CAPRIE. Cerebrovasc Dis 1999; 9(suppl 1): <0.60 (n=25) 0.60-<0.70 (n=21) 1.0-<1.10 (n=980) 0.70-<0.80 (n=40) 0.80-<0.90 (n=130) 0.90-<1.0 (n=195) Kiindulási boka-kar index. *Az átlagos követési idő 8.3 év. Resnick HE et al. Circulation 2004; 109:")
11
Új kardiovaszkuláris rizikó ekvivalensek
>20% a 10 éven belüli kardiovaszkuláris rizikó (a Framingham score alapján) Diabetes mellitus Más formája a klinika atherosclerotikus elváltozásoknak a., perifériás artéria szűkülete b., abdominális aorta aneurysma c., carotis arteria szűkülete Expert Panel on Detection, Evaluation and Treatment of HIgh Blood Cholesterol in Adult. JAMA 2001;285:
 Diabetes mellitus. Más formája a klinika atherosclerotikus elváltozásoknak. a., perifériás artéria szűkülete. b., abdominális aorta aneurysma. c., carotis arteria szűkülete. Expert Panel on Detection, Evaluation and Treatment of HIgh Blood Cholesterol in Adult. JAMA 2001;285:")
12
Relatív 5 éves halálozás
A halálozás nagyon magas súlyos PAD betegekben Relatív 5 éves halálozás Betegek (%) 5 10 15 20 25 30 35 40 45 50 Vastagbél daganat1 Emlő daganat1 Súlyos PAD2 Non-Hodgkin lymphoma3 38 44 48 Mortality is very high in patients with severe PAD Risk of death associated with peripheral arterial disease (PAD) is as high as for many common cancers.1 In a US study of 744 patients tested for PAD, those with severe PAD (ABI < 0.4) had a 5-year survival probability of only 56%.2 This is comparable to the 52% survival in white patients with non-Hodgkin’s lymphoma, as recorded from 1986–1993 by Ries et al.3 Data for colon and breast cancer are reported in the same source. References: 1. Criqui MH. Peripheral arterial disease - epidemiological aspects. Vasc Med 2001; 6 (suppl 1): 3–7. 2. McKenna M et al. The ratio of ankle and arm arterial-pressure as an independent predictor of mortality. Atherosclerosis 1991; 87: 119–128. 3. Ries LAG et al. (Eds). SEER Cancer Statistics Review, 1973–1997. US: National Cancer Institute; 2000. 1. Criqui MH. Vasc Med 2001; 6 (suppl 1): 3–7. 2. McKenna M et al. Atherosclerosis 1991; 87: 119–28. 3. Ries LAG et al. (eds). SEER Cancer Statistics Review, 1973–1997. US: National Cancer Institute; 2000.
 Vastagbél daganat1. Emlő. daganat1. Súlyos. PAD2. Non-Hodgkin. lymphoma Mortality is very high in patients with severe PAD. Risk of death associated with peripheral arterial disease (PAD) is as high as for many common cancers.1 In a US study of 744 patients tested for PAD, those with severe PAD (ABI < 0.4) had a 5-year survival probability of only 56%.2 This is comparable to the 52% survival in white patients with non-Hodgkin’s lymphoma, as recorded from 1986–1993 by Ries et al.3 Data for colon and breast cancer are reported in the same source. References: 1. Criqui MH. Peripheral arterial disease - epidemiological aspects. Vasc Med 2001; 6 (suppl 1): 3–7. 2. McKenna M et al. The ratio of ankle and arm arterial-pressure as an independent predictor of mortality. Atherosclerosis 1991; 87: 119– Ries LAG et al. (Eds). SEER Cancer Statistics Review, 1973–1997. US: National Cancer Institute; Criqui MH. Vasc Med 2001; 6 (suppl 1): 3–7. 2. McKenna M et al. Atherosclerosis 1991; 87: 119– Ries LAG et al. (eds). SEER Cancer Statistics Review, 1973–1997. US: National Cancer Institute;")
13
A perifériás érbetegség diagnózisa az elsődleges ellátás alapja
- A perifériás érbetegség diagnózisa az elsődleges ellátás alapja Az agresszív rizikócsökkentés egyik fontos eleme a PAD kezelésének A kezelés másik fontos célja a PAD progresszió csökkentése, illetve a PAD kialakulás megakadályozása PAD: A Call to Action The objective of this slide kit is to help primary care physicians (PCPs) recognise PAD and to raise awareness amongst PCPs that PAD is a risk marker for broader more serious risk; a patient who is diagnosed with PAD is at high risk of life-threatening cardiovascular and cerebrovascular ischemic complications This slide kit has been developed in response to the ‘PAD Call to Action’ Paper. The paper was written by a group of medical experts who wanted to extend this important message about PAD to the broad medical community1. This slide kit aims in particular to put into action four of the items called for in this paper: Increase awareness of PAD and its consequences (serious future cardiovascular and cerebrovascular complications) Improve the identification of patients with symptomatic PAD Improve treatment rates among patients who have been diagnosed with symptomatic PAD Increase the rates of early detection among the asymptomatic population Reference: Belch JJ et al. Critical issues in peripheral arterial disease detection and management. Arch Intern Med 2003; 163: 884 – 892.
 recognise PAD and to raise awareness amongst PCPs that PAD is a risk marker for broader more serious risk; a patient who is diagnosed with PAD is at high risk of life-threatening cardiovascular and cerebrovascular ischemic complications. This slide kit has been developed in response to the ‘PAD Call to Action’ Paper. The paper was written by a group of medical experts who wanted to extend this important message about PAD to the broad medical community1. This slide kit aims in particular to put into action four of the items called for in this paper: Increase awareness of PAD and its consequences (serious future cardiovascular and cerebrovascular complications) Improve the identification of patients with symptomatic PAD. Improve treatment rates among patients who have been diagnosed with symptomatic PAD. Increase the rates of early detection among the asymptomatic population. Reference: Belch JJ et al. Critical issues in peripheral arterial disease detection and management. Arch Intern Med 2003; 163: 884 – 892.")
14
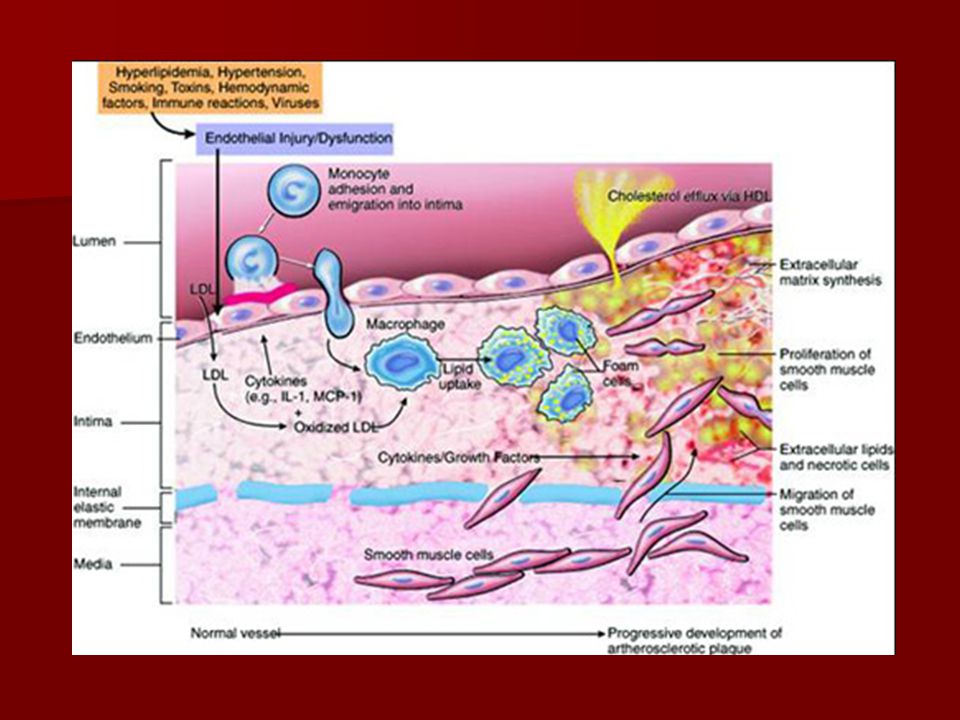
Érelmeszesedéses szűkület thrombussal
Lipidben gazdag sejtek Pathological studies have shown that rupture of atherosclerotic plaques and subsequent luminal thrombosis underlies the aetiology of acute ischaemic coronary syndromes, including myocardial infarction and unstable angina. A lipid-rich core (particularly in the shoulder regions of lesions), abundance of inflammatory cells, a thin fibrous cap and dysfunctional overlying endothelium characterise morphological features of lesions prone to rupture. Dysfunctional endothelium may contribute to the propensity of plaque rupture owing to its pro-inflammatory, prothrombotic and vasoconstrictive properties that modulate lesion composition, growth responses, vascular tone and local shear stress.1 Reference 1. Ross R. N Engl J Med 1999;362:115–126.
, abundance of inflammatory cells, a thin fibrous cap and dysfunctional overlying endothelium characterise morphological features of lesions prone to rupture. Dysfunctional endothelium may contribute to the propensity of plaque rupture owing to its pro-inflammatory, prothrombotic and vasoconstrictive properties that modulate lesion composition, growth responses, vascular tone and local shear stress.1. Reference. 1. Ross R. N Engl J Med 1999;362:115–126.")
15
A fizikai aktivitás hatékonyságát 20 kontrollált tanulmány igazolta.
A fizikai aktivitás 179%-kal növelte a claudicatios távolságot 21 tanulmány metaanalízise alapján. A legkedvezőbb hatást akkor észlelték, amikor az egyes aktivitások időtartama hosszabb volt, mint 30 perc és hetente legalább három alkalommal végezték és a betegek közel a maximális fájdalmat elérték minden egyes mozgás során. Ohta T: Vasa 2002;31:23-7., Gardner AW: J Cardiopulm Rehabil 2002;22:192-8. Langbein WE: J Vasc Surg 2002;35: Stewart KJ: N Engl J Med 2002;347: Stewart KJ: N Engl J Med: 2002;347: Stewart KJ: N Engl J Med: 2002;347:

16
Az alsóvégtagi perifériás érbetegségek konzervatív kezelése
Kardiovaszkuláris rizikó-csökkentés a., lipidcsökkentő kezelés b., vérnyomáscsökkentés c., diabetes mellitus kezelése d., dohányzás megszüntetése e., homocystein csökkentése f., thrombocyta-aggregáció-gátló és antithromboticus kezelés

17
Különböző, nagy klinikai tanulmányok bizonyították azt, hogy a lipidcsökkentő terápia alkalmazása olyan perifériás érbetegeknél akiknek coronaria, vagy cerebrovascularis betegsége van, előnyös A HPS tanulmányban a 40 mg simvastatin alkalmazása jelentős mértékben csökkentette a cardiovascularis ischaemias eseményeket a perifériás érbetegségben szenvedő csoportban annak ellenére, hogy a kiindulási LDL-cholesterin szintjük alacsony volt. LaRosa JC: JAMA 1999; , Ansell BJ: JAMA 1999;282: , Elam MB: JAMA 2000;284: , Blankenhorn DH: Circulation 1991;83: , Buchwald H: Surgery 1996;120:672-9., Duffield RG: Lancet 1983;2: , Buchwald H: N Engl J Med: 1990;323: Pedersen TR: AM J Cardiol 1998;81:333-5., Heart Protection Study Collaborative Group. Lancet 2002;360:7-22.

18
A jelenlegi ajánlás perifériás érbetegeknél:
A lipid szintek normalizálása csökkenti a progressziót és a claudicatio súlyosságát A jelenlegi ajánlás perifériás érbetegeknél: LDL-cholesterin >2.6 mmol/l Triglycerid >3.9 mmol/l Statinokat kell alkalmazni kezdő terápiaként. Az acido-nikotinicum szintén alkalmazható, mivel növeli a HDL szintet, csökkenti a triglycerid szintet LaRosa JC: JAMA 1999; , Ansell BJ: JAMA 1999;282: Elam MB: JAMA 2000;284: , Blankenhorn DH: Circulation 1991;83: Buchwald H: Surgery 1996;120:672-9., Duffield RG: Lancet 1983;2: Buchwald H: N Engl J Med: 1990;323: , Pedersen TR: AM J Cardiol 1998;81:333-5., Heart Protection Study Collaborative Group. Lancet 2002;360:7-22. Elam MB: JAMA 2000;284:

19
Átlagos LDL-C-csökkenés (%)
REVERSAL = 50%-nál nagyobb LDL-C-csökkenéssel megállítható az atherosclerosis progressziója 20 15 10 atheroma térfogatában (mm3) Átlagos változás az 5 –5 A REVERSAL (Reversal of Atherosclerosis with Agressive Lipid Lowering) Study alapján az 50%-ot meghaladó LDL-C csökkenés esetén megállhat, sőt vissza is fordulhat az atherosclerosis folyamata. A vizsgálatban 80 mg atorvastatint hasonlítottak összes 40 mg pravastatinnal és az atherosclerosis progressióját intravascularis UH-gal monitorozták. –10 –80 –70 –60 –50 –40 –30 –20 –10 10 20 Átlagos LDL-C-csökkenés (%) Nissen SE, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis. JAMA. 2004;291:
 Átlagos változás az. 5. –5. A REVERSAL (Reversal of Atherosclerosis with Agressive Lipid Lowering) Study alapján az 50%-ot meghaladó LDL-C csökkenés esetén megállhat, sőt vissza is fordulhat az atherosclerosis folyamata. A vizsgálatban 80 mg atorvastatint hasonlítottak összes 40 mg pravastatinnal és az atherosclerosis progressióját intravascularis UH-gal monitorozták. –10. –80. –70. –60. –50. –40. –30. –20. – Átlagos LDL-C-csökkenés (%) Nissen SE, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis. JAMA. 2004;291:")
20
Az ATPIII módosítására ajánlás
Kockázati kategória Célérték LDL-C mmol/l Koleszterin Nagyon magas Coronaria beteg + diabetes mellitus + erős dohányos + acut coronaria syndroma + metabolikus syndroma 1.8 3.0 Magas ISZB és ISZB ekvivalensek, kockázat > 20% 2.6 4.0 Közepes 2 vagy több rizikófaktor, kockázat <20% 3.4 5.2 Alacsony 0-1 kockázati tényező 4.1 6.5 Grundy SM: J Am Coll Cardiol 2004; 44:

21
a., Lipidcsökkentő kezelés
1.HMG coenzym-A reduktáz-gátló kezelés szükséges minden perifériás érbetegnek 2.6 mmol/l-nél kisebb LDL-C célértéket kell elérni (B típusú evidencia) 2. A nagyon magas rizikójú PAD betegeknél 1.8 mmol/l LDL-C célértéket kell elérni (B típusú evidencia) 3. A fibrátokkal történő kezelés hasznos lehet olyan PAD betegek számára, akiknek a HDL szintjük alacsony, triglyceridjük magas, és LDL-C szintjük normális (C-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:
 2. A nagyon magas rizikójú PAD betegeknél 1.8 mmol/l LDL-C célértéket kell elérni (B típusú evidencia) 3. A fibrátokkal történő kezelés hasznos lehet olyan PAD betegek számára, akiknek a HDL szintjük alacsony, triglyceridjük magas, és LDL-C szintjük normális (C-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:")
22
A cardiovascularis betegségben szenvedő agresszív antihypertensiv kezelésben részesülő PAD betegek vizsgálata alapján a hypertonia a PAD egyik fő rizikófaktora, de az antihypertensiv kezelés hatása a betegség progressziójára nem teljesen világos. Regensteiner JG: AM J Med 2002;112:49-57.

23
c., Diabetes mellitus kezelése
Megfelelő lábápolás, megfelelő cipő viselése, napi lábellenőrzés, a láb bőrének hidratáló krémmel való kezelése szükséges. És a meglévő bőrlaesiók, fekélyek sürgős kezelése javasolt PAD betegeknél. (B-típusú evidencia) A diabeteses PAD betegeknél a HbA1C szint<7% legyen, mely csökkenti a microvascularis szövődményeket és a kardiovaszkuláris rizikót (C-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:
 A diabeteses PAD betegeknél a HbA1C szint<7% legyen, mely csökkenti a microvascularis szövődményeket és a kardiovaszkuláris rizikót (C-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:")
24
Koszorúér vasoconstrictio thrombocyta aggregatio Nikotin
Dohányzás Koszorúér vasoconstrictio thrombocyta aggregatio Nikotin hogy a nikotin fokozza az erek összehúzódását a thrombocyta aggregációt, valamint a dohányzás során kialakult hypoxia direkt endothel hatása is elősegíti a perifériás érbetegség kialakulását, illetve súlyosbodását. CO Hypoxia

25
A felnőttek ¼-e az Amerikai Egyesült Államokban dohányzik.
A dohányosok 70%-a mondta azt, hogy le akart szokni a dohányzásról. A dohányosok kb. 1/3-a próbál leszokni a dohányzásról évente, de csak 20% kap megfelelő szakmai segítséget. Szakmai segítség nélkül dohányzást abbahagyóknak kevesebb, mint 10%-a képes hosszú időtartamra abbahagyni a dohányzást. A dohányzás megszüntetésének bizonyított hatékony módszere a gyógyszeres kezelés és a tanácsadás. Külön-külön is effektívek, de kombináltan alkalmazva jóval nagyobb a leszokás gyakorisága. Rigotti NA: N Engl J Med 2002;346: Rigotti NA: N Engl J Med 2002;346: Rigotti NA: N Engl J Med 2002;346: JAMA 2000;283: Krupski WC: J Vasc Surg 2002;36: Rigotti NA: N Engl J Med 2002;346: Krupski WC: J Vasc Surg 2002;36:

26
A dohányzás az egyik legfontosabb rizikófaktora a PAD-nak.
Korábbi metaanalízis szerint a dohányzás megszüntetése csökkenti a claudicatio súlyosságát A dohányzás abbahagyása csökkenti a betegség progresszióját az amputáció gyakoriságát és az ischaemias tüneteket, ezen kívül a myocardialis infarctust és a vascularis halálozást Regensteiner JG: AM J Med 2002;112:49-57. Girolami B: Arch Intern Med 1999;159: Girolami B: Arch Intern Med 1999;159:

27
d., Dohányzás megszüntetése
1. A perifériás érbetegségben szenvedő dohányosoknál a dohányzás minél előbbi megszüntetése javasolt, melyet életmód-változtatással, nikotinpótló kezeléssel vagy bupropion adásával érünk el (B-típusú evidencia) Bupropion (amfebutamone) szelektív serotonin reuptake-gátló, antidepresszáns. (Wellbutrin, Zyban néven van forgalomban) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:
 Bupropion (amfebutamone) szelektív serotonin reuptake-gátló, antidepresszáns. (Wellbutrin, Zyban néven van forgalomban) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:")
28
A Ticlid-el végzett randomizált tanulmányok igazolták azt, hogy javítja a claudicatios távolságot és csökkenti az occlusiot Ezt hosszabb ideig nem használják, mivel életveszélyes hematológiai reakciókat vált ki. Regensteiner JG: AM J Med 2002;112:49-57. Hiatt WR: N Engl J Med 2001;344:

29
f., Thrombocyta-aggregáció-gátló és antithromboticus kezelés
A thrombocyta-gátló kezelés csökkenti az AMI-t, stroke-ot, a vascularis halálozást a PAD betegekben (A-típusú evidencia) mg/napi Aspirin dózis javasolt az AMI, a stroke és a vascularis halálozás csökkentésére PAD betegeknél (A-típusú evidencia) 75 mg/nap dózisban alkalmazott clopidogrel az ajánlott helyettesítője az Aspirin kezelésnek az AMI, stroke, vagy a vascularis halálozás csökkentésére PAD betegeknél (B-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:
 mg/napi Aspirin dózis javasolt az AMI, a stroke és. a vascularis halálozás csökkentésére PAD betegeknél (A-típusú evidencia) 75 mg/nap dózisban alkalmazott clopidogrel az ajánlott. helyettesítője az Aspirin kezelésnek az AMI, stroke, vagy a vascularis halálozás csökkentésére PAD betegeknél (B-típusú evidencia) ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease . J Vasc Interv Radiol 2006;17:")
30
f., Thrombocyta-aggregáció-gátló és antithromboticus kezelés
A warfarin kezelés nem csökkentette a vascularis ischaemias eseményeket PAD betegekben (C-típusú evidencia)
")
31
A claudicatio gyógyszeres kezelése
Pentoxifyllin 3x400 mg/nap másodsorban a cilostazol alternatíváját jelentő kezelés claudicatio intermittensben csökkenti a claudicatios távolságot (A-típusú evidencia) A pentoxifyllin klinikai hatékonysága a claudicatiora csekély és nem teljesen bizonyított (C típusú evidencia)
 A pentoxifyllin klinikai hatékonysága a claudicatiora csekély és nem teljesen bizonyított (C típusú evidencia)")
32
A claudicatio gyógyszeres kezelése
Ginkgo biloba Ginkgo pótlók dózisa mg/nap kismértékben javítja a claudicatios távolságot, nem teljesen bizonyított (B-típusú evidencia) A Ginkgo levél kivonata Flavonoid glycosidot, ginkgolidot tartalmaz. Antioxidáns, thrombocyta-gátló és a microcirculatio javító hatása miatt használják. Mellékhatás: vérzés fokozás, gastrointestinalis dyscomfort-érzés, hányinger, hányás, fejfájás, szédülés.
 A Ginkgo levél kivonata Flavonoid glycosidot, ginkgolidot tartalmaz. Antioxidáns, thrombocyta-gátló és a microcirculatio javító hatása miatt használják. Mellékhatás: vérzés fokozás, gastrointestinalis dyscomfort-érzés, hányinger, hányás, fejfájás, szédülés.")
Hasonló előadás