Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Akut Leukaemia

2
Blood Cell Formation

3
CMP MEPMEP BMCPBMCP hízósejthízósejt basophil thrombocyta erythrocyta ST-HSC Őssejt >16 hétig LT-HSC 6-8 hétig Haematopoiesis GMP monocyta/ macrophag eosinophil neutrophil TNKP BCPBCP T-sejt B-sejt NK-sejt CLPCLP dendriticus sejt önmegújít vérképzést biztosít MPP 2-6 hétig aktív LT-HSC nyugvó LT-HSC „myeloid” LT-HSC „lymphoid” LT-HSC

4
CMP MEPMEP BMCPBMCP hízósejthízósejt basophil thrombocyta erythrocyta ST-HSC LT-HSC MYELOID Haematopoiesis GMP monocyta/ macrophag eosinophil neutrophil TNKP BCPBCP T-sejt B-sejt NK-sejt CLPCLP MMP dendriticus sejt LYMPHOID HISTIOCYTÁS

5
Hematopoietic stem cell Neutrophils Eosinophils Basophils Monocytes Platelets Red cells Myeloid progenitor Lymphoid progenitor B-lymphocytes T-lymphocytes Plasma cells naïve ALL AML

6
Leukaemia Malignant Transformation Malignant Transformation Proliferation & Accumulation Proliferation & Accumulation ↙ ↘ Peripheral blood → Blasts in BM Peripheral blood → Blasts in BM Visceral organs Cytopenias Visceral organs Cytopenias

7
Acute Leukaemia accumulation of blasts in the marrow

8
FAB vs WHO Classifications of Haematologic Neoplasms FAB criteriaFAB criteria –Morphology –Cytochemistry WHO criteriaWHO criteria –Morphology –Immunophenotyping –Genetic features KaryotypingKaryotyping Molecular testingMolecular testing –Clinical features

9
Acute Leukaemia A clonal, molecular abnormality of hematopoietic blast cells resulting in a failure of differentiation & uncontrolled cell proliferation Accumulation of leukaemic blast cells results in marrow replacement, organ infiltration and metabolic effects

10
Akut leukaemia Malignus össejt betegség, érési zavar, kiszorítja az érett csontvelőt Legtöbbször ismeretlen ok, de besugárzás, benzol, egyes cytostatikumok: alkiláló szerek Az akut lymphoid leukaemia (ALL) gyermekek betegsége, az akut myeloid leukaemia (AML) 60 év körül jelentkezik
 gyermekek betegsége, az akut myeloid leukaemia (AML) 60 év körül jelentkezik")
11
Akut leukaemia Haemopoietikus rendszer klonális megbetegedése, melyben a kóros sejtek haemopoeticus őssejtből, vagy valamely myeloid vagy lymphoid sejtvonal irányába elkötelezett őssejtből származnak Éretlen elemek (blastok) felszaporodása és az érett sejtek számának jelentős csökkenése jellemzi Diagnosztikus kritérium: csontvelőben és/vagy perifériás vérben a blastok vagy blastekvivalens sejtek aránya 20% vagy annál nagyobb
 felszaporodása és az érett sejtek számának jelentős csökkenése jellemzi Diagnosztikus kritérium: csontvelőben és/vagy perifériás vérben a blastok vagy blastekvivalens sejtek aránya 20% vagy annál nagyobb")
12
Akut leukaemia Magyarországon évente kb. 300 új AML Többségük idős, átlagos életkor 65 év körül Férfiak:nők 1:1 Felnőttkorban akut leukémiák 70-80% Gyermekkorban 15% Családi halmozódás ritka Betegség oka ismeretlen (kivéve daganatellenes terápiában részesülők) A betegek többsége az első évben meghal, vagy meggyógyul
 A betegek többsége az első évben meghal, vagy meggyógyul.")
13
Leukaemia A z AML a felnőttkori heveny leukaemiás esetek 80%-át teszi ki A betegség felismerésekor a betegek medián életkora 65 év A CHR elérése alapvető feltétel a hosszútávú túléléshez és a gyógyuláshoz A legtöbb fiatal beteg alkalmas az intenzív kemoterápiára, kezelésük kuratív célú A gyógyult betegek aránya kb. 30-40%, amely időskori AML- ben mindössze 10-15 % lehet A rossz prognosis okai: kísérőbetegségek, a kedvezőtlen prognosztikai markerek gyakoribb előfordulása és a kemorezisztencia Az idősebb betegek az intenzív kemoterápiára kevésbé alkalmasak

14
Akut leukaemia Diagnózis alapja a periférás vér és csontvelő aspirátum citológiai vizsgálata Biopsiára ritkán van szüksége (ha a fentiek nem elégségesek) Diagnosztikus kritérium blastok 20% felett 20 % alatt, ha blastok leukaemia specifikus kromoszóma-eltérést hordoznak Auer pálca (myeloid leukaemiára jellemző specifikus eltérés) Pseudo-Chediac-Hirgashi féle citoplazmatikus granuláció-óriás granulumok, azurophil granulomok Csontvelő szövettani vizsgálat- hypocellularis AML és aplasticus anaemia differenciál diagnosztikája Ritkán perifériás vérben blastok hiánya (aleukaemiás leukaemia) Egy részét kifejezett myelofibrosis kíséri- punctio sicca Ritkán tumorszerűen növekvő extramedullartis lokalizáció- chloroma, myelosarcoma (normális csv), későbbiekben csv és perifériás vér is érintett
 Diagnosztikus kritérium blastok 20% felett 20 % alatt, ha blastok leukaemia specifikus kromoszóma-eltérést hordoznak Auer pálca (myeloid leukaemiára jellemző specifikus eltérés) Pseudo-Chediac-Hirgashi féle citoplazmatikus granuláció-óriás granulumok, azurophil granulomok Csontvelő szövettani vizsgálat- hypocellularis AML és aplasticus anaemia differenciál diagnosztikája Ritkán perifériás vérben blastok hiánya (aleukaemiás leukaemia) Egy részét kifejezett myelofibrosis kíséri- punctio sicca Ritkán tumorszerűen növekvő extramedullartis lokalizáció- chloroma, myelosarcoma (normális csv), későbbiekben csv és perifériás vér is érintett")
15
Lab evaluation –The lab diagnosis is based on two things –Finding a significant increase in the number of immature cells in the bone marrow including blasts, promyelocytes, promonocytes (>30% blasts is diagnostic) –Identification of the cell lineage of the leukaemic cells –Peripheral blood: Anaemia (normochromic, normocytic) Decreased platelets Variable WBC count –The degree of peripheral blood involvement determines classification: »Leukaemic – increased WBCs due to blasts »Subleukaemic – blasts without increased WBCs »Aleukaemic – decreased WBCs with no blasts
 –Identification of the cell lineage of the leukaemic cells –Peripheral blood: Anaemia (normochromic, normocytic) Decreased platelets Variable WBC count –The degree of peripheral blood involvement determines classification: »Leukaemic – increased WBCs due to blasts »Subleukaemic – blasts without increased WBCs »Aleukaemic – decreased WBCs with no blasts")
16
Bone marrow in acute leukaemi a Necessary for diagnosis (cytogenetics) Useful for determining type (immunophenotyping) Useful for prognosis (cytogenetics, molecular genetics) Acute leukaemias are defined by the presence of > 20% blasts in bone marrow (% of nucleated marrow cells)
 Useful for determining type (immunophenotyping) Useful for prognosis (cytogenetics, molecular genetics) Acute leukaemias are defined by the presence of > 20% blasts in bone marrow (% of nucleated marrow cells)")
17
Distinguishing AML from ALL Light microscopy –AML: Auer rods, cytoplasmic granules –ALL: no Auer rods or granules Flow cytometry Special stains (cytochemistry)
")
18
Pathophysiology of the Acute Leukaemias Acute leukaemia causes morbidity & mortality through three general mechanisms: Deficiency in normal blood cell number or function Invasion of vital organs with impairment of organ function Systemic disturbances shown by metabolic imbalance

19
Acute Leukaemia: AML vs ALL Adults- 85% of acute leukaemia is AML Children- 85% of acute leukaemia is ALL Leukemic Blast morphology –AML: cytoplasmic granules, Auer rods, more cytoplasm, 2-5 nucleoli –ALL: no cytoplasmic granules, minimal cytoplasm, 1-2 nucleoli

20
Acute Leukaemia AML vs. ALL Cell Surface Markers by Flow cytometry AML CD13, CD33, glycophorin (M 6 ), platelet antigens (M 7 ) ALL B lineage: CD19, CD22, CD10 (+/-), surface Ig, T lineage: CD2, CD3, CD5, CD7
, platelet antigens (M 7 ) ALL B lineage: CD19, CD22, CD10 (+/-), surface Ig, T lineage: CD2, CD3, CD5, CD7.")
21
Acute Leukaemia: AML vs. ALL CytochemistryAMLALL Myeloperoxidase + - Sudan black + - Non-specific esterase + (M 4,5 ) - PAS + (M 6 ) + Acid phosphatase + (M 6 ) +
 - PAS + (M 6 ) + Acid phosphatase + (M 6 ) +.")
22
Flow Cytometry & FISH Analysis

23
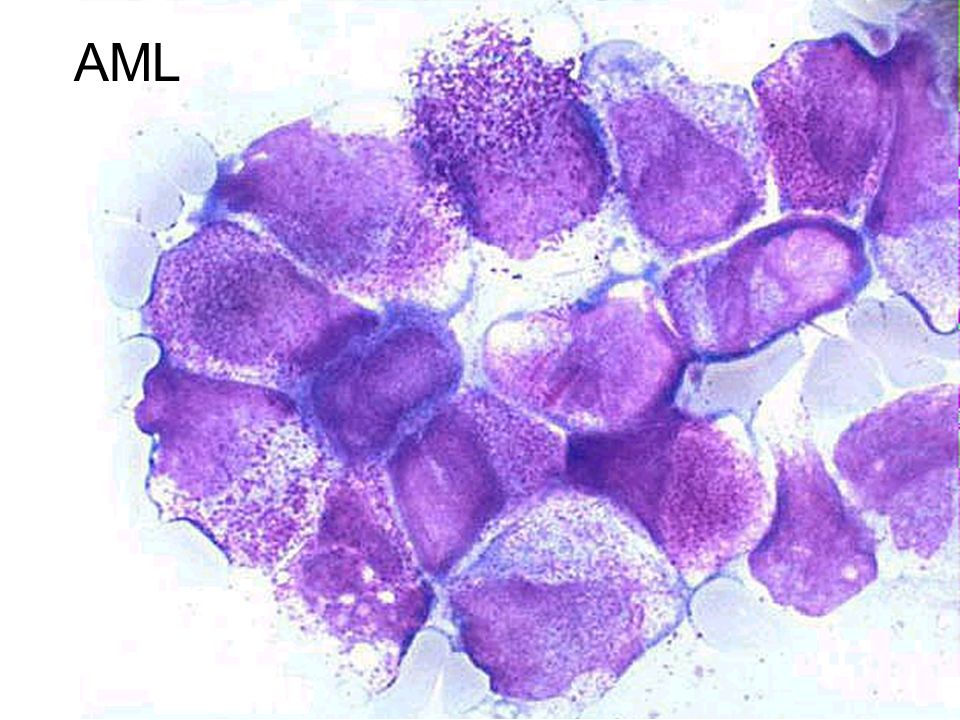
AML AML characterized by proliferation of myeloid tissue & an abnormal increase in the number of myeloblasts in the bone marrow & peripheral bloodAML characterized by proliferation of myeloid tissue & an abnormal increase in the number of myeloblasts in the bone marrow & peripheral blood 25% of all leukaemias25% of all leukaemias –85% of the acute leukaemias in adults Abrupt, dramatic onsetAbrupt, dramatic onset –Serious infections, abnormal bleeding Uncontrolled proliferation of myeloblastsUncontrolled proliferation of myeloblasts –Hyperplasia of bone marrow & spleen

24
AML French-American-British (FAB) Classification M0: Minimally differentiated leukaemia M1: Myeloblastic leukaemia without maturation M2: Myeloblastic leukemia with maturation M3: Hypergranular promyelocytic leukaemia M4Eo: Variant: Increase in abnormal marrow eosinophils M4: Myelomonocytic leukaemia M5: Monocytic leukaemia M6: Erythroleukaemia (DiGuglielmo's disease) M7: Megakaryoblastic leukaemia
 Classification M0: Minimally differentiated leukaemia M1: Myeloblastic leukaemia without maturation M2: Myeloblastic leukemia with maturation M3: Hypergranular promyelocytic leukaemia M4Eo: Variant: Increase in abnormal marrow eosinophils M4: Myelomonocytic leukaemia M5: Monocytic leukaemia M6: Erythroleukaemia (DiGuglielmo s disease) M7: Megakaryoblastic leukaemia")
25
WHO Classification of AML AML with recurrent cytogenetic translocationsAML with recurrent cytogenetic translocations AML with multi-lineage dysplasiaAML with multi-lineage dysplasia AML & myelodysplasia, therapy relatedAML & myelodysplasia, therapy related AML, not otherwise categorizedAML, not otherwise categorized

26
AML myelodysplasiával kapcsolatos eltérésekkel AML visszatérő genetikai eltéréssel t(8;21)(q22;q22) – RUNX1-RUNX1T1 inv(16)(p13q22) – CBFB-MYH11 t(15;17)(q24;q21) – PML-RARA t(9;11)(p22;q23) – MLLT3-MLL t(6;9)(p23;q34) – DEK-NUP214 inv(3)(q21q26) – RPN1-EVI1 Akut myeloid leukaemia - klasszifikáció AML, terápiával összefüggő AML, máshogy nem osztályozott Myeloid sarcoma Down-szindrómához társuló myeloid proliferációk t(1;22)(p13;q13) – RBM15-MKL1 NPM1 mutáció CEBPA mutáció
(q22;q22) – RUNX1-RUNX1T1 inv(16)(p13q22) – CBFB-MYH11 t(15;17)(q24;q21) – PML-RARA t(9;11)(p22;q23) – MLLT3-MLL t(6;9)(p23;q34) – DEK-NUP214 inv(3)(q21q26) – RPN1-EVI1 Akut myeloid leukaemia - klasszifikáció AML, terápiával összefüggő AML, máshogy nem osztályozott Myeloid sarcoma Down-szindrómához társuló myeloid proliferációk t(1;22)(p13;q13) – RBM15-MKL1 NPM1 mutáció CEBPA mutáció")
27
Akut myeloid leukaemia Epidemiológia 60 év az átlagéletkor kb. 3/100.000 incidencia Etiológia ionizáló sugárzás kemoterápia: alkiláló szerek, topoizomeráz gátlók vegyszerek: permetezőszerek, benzol genetikai betegségek: Down, Fanconi anaemia, Bloom, Wiscott-Aldrich, stb. Klinikai kép cytopaenia következmények: gyengeség, infekciók, vérzés extramedullaris manifesztáció

28
AML

30
Auer rods in AML

31
AML Clinical Features & Prognosis Age – 80% remission, 20-30% DFS –> 60 years: ~60% remission, 5-15% DFS Prior marrow disorder: Myelodysplasia (MDS) Secondary AML (prior chemo or radiotherapy) Response to induction therapy
 Secondary AML (prior chemo or radiotherapy) Response to induction therapy")
32
AML Cytogenetics & Prognosis Favorable t(8;21), t(15;17), inv(16) Intermediate (Most patients) normal, +8, +21, +22, del(7q), del(9q), Adverse -5, -7, del(5q), abnormal 3q, complex karyotype (> 3 -5 abnormalities)
, t(15;17), inv(16) Intermediate (Most patients) normal, +8, +21, +22, del(7q), del(9q), Adverse -5, -7, del(5q), abnormal 3q, complex karyotype (> 3 -5 abnormalities)")
33
AML Cytogenetics & Prognosis GroupCR5 year survival Favorable91%65-75% Intermediate86%40-50% Adverse63%<15%

34
AML Mutations & Prognosis Flt 3 (ITD) - Adverse NPM-1 mutation & no Flt3 - Favorable MLL (PTD) - Adverse CEBPA - Favorable
 - Adverse NPM-1 mutation & no Flt3 - Favorable MLL (PTD) - Adverse CEBPA - Favorable")
35
Akut myeloid leukaemia Pedersen-Bjergaard J et al. Leukemia. 2006;20(11): 1943–1949. Molekuláris patogenezis 1es típusú mutáció jelátviteli útvonal – fokozott proliferáció pl.: NRAS/KRAS, FLT3, KIT, JAK2, PTPN11 2es típusú mutáció transzkripciós faktorok – differenciációs zavar pl.: CBF, MLL, NPM1, CEPBA, RUNX1, RARA 3-as típusú mutáció? epigenetikai reguláció – differenciációs zavar pl.: TET2, IDH1/2, DNMT3A, ASXL2, EZH2
: 1943–1949. Molekuláris patogenezis 1es típusú mutáció jelátviteli útvonal – fokozott proliferáció pl.: NRAS/KRAS, FLT3, KIT, JAK2, PTPN11 2es típusú mutáció transzkripciós faktorok – differenciációs zavar pl.: CBF, MLL, NPM1, CEPBA, RUNX1, RARA 3-as típusú mutáció. epigenetikai reguláció – differenciációs zavar pl.: TET2, IDH1/2, DNMT3A, ASXL2, EZH2.")
36
Gum hypertrophy

37
A B C Chloromas NEJM 1998

38
AML – t(15;17) Jellemzők 5-10% AML fiatal felnőtt DIC kedvező prognózis ATRA kezelés differenciációt érhet el myeloblastok 10% körül variáns transzlokációk pl. t(11;17)(q23;q11) már kedvezőtlen hypergranuláris (klasszikus) hypogranuláris (microgranularis): bilobált, hajtogatott – monocytaszerű erős CD33, CD177, de CD34-, HLADR- PML-RARA fúzió, abnormális PML lokalizáció
(q23;q11) már kedvezőtlen hypergranuláris (klasszikus) hypogranuláris (microgranularis): bilobált, hajtogatott – monocytaszerű erős CD33, CD177, de CD34-, HLADR- PML-RARA fúzió, abnormális PML lokalizáció.")
39
AML Treatment: Induction Chemotherapy Anthracycline (Idarubicin) for 3 days & Cytosine arabinoside (Ara-C) for 7 days (3+7, Younger/fit patients only) DAT (Daunorubicin, Cytosine Arabinoside, Thioguanine) Three to 5 weeks of pancytopenia Supportive care red cell & platelet transfusions, prophylactic antibacterial, antifungals & antivirals
 for 3 days & Cytosine arabinoside (Ara-C) for 7 days (3+7, Younger/fit patients only) DAT (Daunorubicin, Cytosine Arabinoside, Thioguanine) Three to 5 weeks of pancytopenia Supportive care red cell & platelet transfusions, prophylactic antibacterial, antifungals & antivirals")
40
AML: Response to Ind uction Remission status determined by bone marrow at end of induction therapy (days 14-28) Complete haematological remission: –Normal peripheral blood counts –Normocellular marrow with < 5% blasts & normal marrow cell maturation
 Complete haematological remission: –Normal peripheral blood counts –Normocellular marrow with < 5% blasts & normal marrow cell maturation")
41
AML Treatment: Consolidation Following induction into Complete Remission Double induction (e.g. HAM) 4 cycles of high dose cytosine arabinoside (HiDAC) administered approximately every 5-6 weeks OR Bone marrow (peripheral blood stem cell) transplant (Depends on degree of risk)
 4 cycles of high dose cytosine arabinoside (HiDAC) administered approximately every 5-6 weeks OR Bone marrow (peripheral blood stem cell) transplant (Depends on degree of risk).")
42
AML Treatment: Alternative Consolidation One or more cycles of consolidation chemotherapy then either: Autologous stem cell transplant after high dose chemotherapy or Allogeneic bone marrow transplantation after high dose chemotherapy

43
AML Treatment: Autologous Transplant Advantage Collection and subsequent infusion of patient’s stem cells allows administration of otherwise lethal doses of chemotherapy Disadvantages Despite CR, leukaemic cells may persist in marrow, blood & stem cell product High dose therapy more toxic than standard consolidation

44
AML Treatment: Allogeneic Transplant Advantages Stem cells from HLA-matched sibling or unrelated individual allow high dose therapy & are free of leukaemia Immunologic graft versus leukaemia effect (GVL) Results in decreased rate of leukaemic relapse
 Results in decreased rate of leukaemic relapse")
45
AML Treatment: Allogeneic Transplant Disadvantages –Immunologic graft versus host disease (GVHD) and immunosuppressive therapy result in significant morbidity & mortality –GVHD incidence & severity increases with increasing age (Best results in Pediatrics) –Tolerability of high dose transplant limited by patient age (RIC)
 and immunosuppressive therapy result in significant morbidity & mortality –GVHD incidence & severity increases with increasing age (Best results in Pediatrics) –Tolerability of high dose transplant limited by patient age (RIC)")
46
AML Treatment: A risk adapted approach Favorable Conventional chemotherapy followed by transplant only if relapse occurs Intermediate Conventional chemotherapy alone or autologous or allogeneic transplant Adverse Conventional chemotherapy followed by allogeneic transplant

47
Current Risk Stratification OHSU Acute Leukemia Program Risk StatusCytogeneticsMolecular Mutations Better-riskInv(16) 1 t(8 ;21) 1 t(16 ;16) 1 Normal cytogenetics with isolated NPM 1 mutation Intermediate-riskNormal +8 only t(9 ;11) MK negative c-KIT 3 in patients with t(8;21) or Inv(16) Poor-riskComplex (>3 abnormalities) -5, -7, 5q-, 7q- MK positive Normal cytogenetics with isolated FLT3 mutations
 1 t(8 ;21) 1 t(16 ;16) 1 Normal cytogenetics with isolated NPM 1 mutation Intermediate-riskNormal +8 only t(9 ;11) MK negative c-KIT 3 in patients with t(8;21) or Inv(16) Poor-riskComplex (>3 abnormalities) -5, -7, 5q-, 7q- MK positive Normal cytogenetics with isolated FLT3 mutations")
48
Hematopoietic stem cell Neutrophils Eosinophils Basophils Monocytes Platelets Red cells Myeloid progenitor Lymphoid progenitor B-lymphocytes T-lymphocytes Plasma cells naïve ALL AML

49
ALL Most common type of leukaemia in childrenMost common type of leukaemia in children 15-20% of acute leukaemia in adults15-20% of acute leukaemia in adults Immature lymphocytes proliferate in the bone marrow& peripheral blood & lymphaticsImmature lymphocytes proliferate in the bone marrow& peripheral blood & lymphatics Signs and symptoms may appear abruptlySigns and symptoms may appear abruptly –Fever, bleeding Insidious with progressiveInsidious with progressive –Weakness, fatigue CNS manifestationsCNS manifestations

50
B cell maturation

51
T cell maturation

52
Precursor T-sejtes lymphoma/leukaemia Akut lymphoblastos leukémia (lymphoblastos lymphoma) Epidemiológia precursor sejtes leukémiák 80-85%-a, a lymphomák 10%-a B-sejtes betegek 75%-a 6 év alatti Tünetek leukémia – mint a B-sejtes lymphoma – jellemzően mediastinalis térfoglalás Morphologia diffúz lymphoblastos infiltráció CD3+, TdT+, CD34+ Genetika TCRα (14q11), TCRβ (7q35) transzlokáció legtöbbször homeobox génekkel
 Epidemiológia precursor sejtes leukémiák 80-85%-a, a lymphomák 10%-a B-sejtes betegek 75%-a 6 év alatti Tünetek leukémia – mint a B-sejtes lymphoma – jellemzően mediastinalis térfoglalás Morphologia diffúz lymphoblastos infiltráció CD3+, TdT+, CD34+ Genetika TCRα (14q11), TCRβ (7q35) transzlokáció legtöbbször homeobox génekkel")
53
ALL

54
WHO Classification of ALL Precursor lymphoid neoplasmsPrecursor lymphoid neoplasms T-cell lymphoblastic leukaemia/lymphomaT-cell lymphoblastic leukaemia/lymphoma B-cell lymphoblastic leukaemia/lymphoma, NOSB-cell lymphoblastic leukaemia/lymphoma, NOS B-cell lymphoblastic leukaemia/lymphoma with recurrent genetic abnormalitiesB-cell lymphoblastic leukaemia/lymphoma with recurrent genetic abnormalities –t(9;22)(q34;q11.2);BCR-ABL1 –t(v;11q23);MLL rearranged –t(12;21)(p13;q22);TEL-AML1(ETV6-RUNX1) –with hyperploidy –With hypoploidy (hypodiploid ALL) –t(5;14)(q31;q32);IL3-IGH –t(1;19)(q23;p13.3);E2A-PBX1 (TCF3-PBX1)
(q34;q11.2);BCR-ABL1 –t(v;11q23);MLL rearranged –t(12;21)(p13;q22);TEL-AML1(ETV6-RUNX1) –with hyperploidy –With hypoploidy (hypodiploid ALL) –t(5;14)(q31;q32);IL3-IGH –t(1;19)(q23;p13.3);E2A-PBX1 (TCF3-PBX1)")
55
IndicatorsFavorablePoor WBC < 50,000/ L 50,000/ L Age1 - 10 < 1 or 10 GenderFemaleMale BlastB-cellT-cell and mixed KaryotypeHyperploidy Trisomy 4, 10, 17 t(12;21) (TEL/AML1) Hypoploidy Trisomy 5 t(1;19 (E2A/PBX1) Mixed lineage leukemia T(9;22) (Ph) BM blast count during induction Marked reduction at day 7 Mild reduction at day 7 Prognosis
 (TEL/AML1) Hypoploidy Trisomy 5 t(1;19 (E2A/PBX1) Mixed lineage leukemia T(9;22) (Ph) BM blast count during induction Marked reduction at day 7 Mild reduction at day 7 Prognosis")
56
Risk classification in ALL 1. Standard risk 2. High risk 3. Very high risk

57
High-risk ALL 1. Pre – T (cCD3+/CD7+/CD2+) 2. Pro – B (CD19+/TdT+/CD10-/cIgG-) 3. Age > 35 years, 4. -WBC > 30 G/L in B-ALL > 100 G/L in T-ALL 5. No remission after 4 weeks of induction therapy therapy 6. Detection of MRD (minimal residual disease) with flow 6. Detection of MRD (minimal residual disease) with flow cytometry or molecular methods- MRD positivity cytometry or molecular methods- MRD positivity 7. t(4;11) 7. t(4;11)
 with flow 6. Detection of MRD (minimal residual disease) with flow cytometry or molecular methods- MRD positivity cytometry or molecular methods- MRD positivity 7. t(4;11) 7. t(4;11).")
58
Collaborative care Goal is to attain remission (when there is no longer evidence of cancer cells in the body) Chemotherapeutic treatment –Induction therapy Attempt to induce or bring remission Seeks to destroy leukaemic cells in the tissues, peripheral blood, bone marrow Patient may become critically ill –Provide psychological support as well
 Chemotherapeutic treatment –Induction therapy Attempt to induce or bring remission Seeks to destroy leukaemic cells in the tissues, peripheral blood, bone marrow Patient may become critically ill –Provide psychological support as well")
Hasonló előadás









 KEZELÉS EREDMÉNYESSÉGÉT BEFOLYÁSOLÓ TÉNYEZŐK KRÓNIKUS LYMPHOID LEUKAEMIÁS (CLL) BETEGEINKBEN FACTORS PREDICTING.>")
, Szendrei Tamás(1), Skrapits Judit(2),>")

Népegészségügyi orvostan 140 és/vagy 90 Hgmm-t elérő és az.>")





 2017. május-június.>")
