Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
A RAAS-gátlás vérnyomáscsökkentéstől független terápiás hatásai
Prof. Dr. Sonkodi Sándor egyetemi tanár Szegedi Tudományegyetem ÁOK I. sz. Belgyógyászati Klinika, Szeged

2
A RAAS-GÁTLÁS VÉRNYOMÁS CSÖKKENTÉSTŐL FÜGGETLEN TERÁPIÁS HATÁSAI
Sonkodi Sándor SzTE, ÁOK, I.sz. Belklinika Nephrologia-Hypertonia Centrum

3
Gradman, A. H. et al. J Am Coll Cardiol 2008;51:519-528
The Renin-Angiotensin Cascade and the 3 Available Approaches to Pharmacologic Inhibition of Production or Action of Angiotensin II Gradman, A. H. et al. J Am Coll Cardiol 2008;51:

4
RAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás Új diabetes kialakulását csökkentik BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

5
PROTEINURIA AND RISK OF DEVELOPING ESRD
Community-based screening in 106,177 general population Follow-up: 17 years 16 14 12 10 Cumulative incidence of ESRD (%) 8 6 4 2 Proteinuria Number of screened Number of ESRD - 86,253 185 + 10,000 38 + 4,007 55 2+ 1,072 76 >3+ 357 55 Iseki et al., Kidney Int, 2003
 Proteinuria. Number of screened. Number of ESRD. - 86, , , , > Iseki et al., Kidney Int,")
6
Probability of Survival
Proteinuria Is an Independent Risk Factor for All-Cause Mortality in Type 2 Diabetes 1.0 Normoalbuminuria (n=191) 0.9 Microalbuminuria (n=86) 0.8 Probability of Survival 0.7 Macroalbuminuria (n=51) Proteinuria Is an Independent Risk Factor for All-Cause Mortality in Type 2 Diabetes The impact of microalbuminuria and macroalbuminuria on all-cause mortality was evaluated by Gall and colleagues, who followed 3 groups of patients with type 2 diabetes for 5 years, dividing them into groups characterized by degree of proteinuria Normoalbuminuria (urine albumin excretion rate [UAER] <30 mg/24 hours Microalbuminuria (UAER 30 to 299 mg/24 hours) Macroalbuminuria (UAER 300 mg/24 hours) From 1987 until January 1993, 8% of patients with normoalbuminuria, 20% of patients with microalbuminuria, and 35% of patients with macroalbuminuria died, predominantly from cardiovascular disease Elevated UAER was associated with increased all-cause mortality risk Reference: Gall MA, Borch-Johnsen K, Hougaard P, et al. Albuminuria and poor glycemic control predict mortality in NIDDM. Diabetes. 1995;44: 0.6 0.5 1 2 3 4 5 6 Years P<0.01 normoalbuminuria vs microalbuminuria and macroalbuminuria. P<0.05 microalbuminuria vs macroalbuminuria. Gall MA et al. Diabetes. 1995;44:
 0.9. Microalbuminuria. (n=86) 0.8. Probability of Survival Macroalbuminuria. (n=51) Proteinuria Is an Independent Risk Factor for All-Cause Mortality. in Type 2 Diabetes. The impact of microalbuminuria and macroalbuminuria on all-cause mortality was evaluated by Gall and colleagues, who followed 3 groups of patients with type 2 diabetes for 5 years, dividing them into groups characterized by degree of proteinuria. Normoalbuminuria (urine albumin excretion rate [UAER] <30 mg/24 hours. Microalbuminuria (UAER 30 to 299 mg/24 hours) Macroalbuminuria (UAER 300 mg/24 hours) From 1987 until January 1993, 8% of patients with normoalbuminuria, 20% of patients with microalbuminuria, and 35% of patients with macroalbuminuria died, predominantly from cardiovascular disease. Elevated UAER was associated with increased all-cause mortality risk. Reference: Gall MA, Borch-Johnsen K, Hougaard P, et al. Albuminuria and poor glycemic control predict mortality in NIDDM. Diabetes. 1995;44: Years. P<0.01 normoalbuminuria vs microalbuminuria and macroalbuminuria. P<0.05 microalbuminuria vs macroalbuminuria. Gall MA et al. Diabetes. 1995;44:")
7
BENAZEPRIL + VALSARTAN
EFFECTS ON PROTEINURIA OF 8 WEEKS COMPARABLE BLOOD PRESSURE CONTROL ACHIEVED BY COMBINED THERAPY IN 63 PATIENTS WITH CHRONIC NON-DIABETIC NEPHROPATHIES BENAZEPRIL + VALSARTAN ( mg/day) 10 BENAZEPRIL (20 mg/day) VALSARTAN (160 mg/day) -10 -20 Percent change from baseline -30 -40 24 hrs Uprot excretion MAP -50 p = 0.022 -60 p = 0.024 -70 p = 0.002 Campbell et al., 2002
 10. BENAZEPRIL. (20 mg/day) VALSARTAN. (160 mg/day) Percent change from baseline hrs Uprot excretion. MAP p = p = p = Campbell et al.,")
8
COOPERATE Trial Hypertensive and Diabetic Nephropathy Patinents (n=383)
140 Combination Trandolapril Losartan 130 120 110 100 Blood pressure (mm Hg) 90 80 70 60 5 10 15 20 25 30 35 40 Baseline Months after randomization Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):
 Baseline. Months after randomization. Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):")
9
COOPERATE Trial Hypertensive and diabetic nephropathy patients
1 2 3 5 10 15 20 25 30 35 40 Months after randomization Median urinary protein excretion (g/day) Combination Trandolapril Losartan Baseline Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):
 Combination. Trandolapril. Losartan. Baseline. Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):")
10
Aliskiren Prevents Albuminuria and Inhibits Renal Inflammation in dTGR

11
RAS-GÁTLÁS - PROTEINURIA
ARB-k és ACE-gátlók mono-terápiában egyformán csökkentik a prooteinuriát, erősebben, mint a CCB-k, v. beta-blokkolók Az ARB és ACE-gátló kombinációja erősebben csőkkenti, mint a két szeré külön-külön Az Aliskerin legalább olyan erős csökkentő, mint a két másik szer, valószínűleg erősebben Th.: - valamelyik RAS- blokkoló adása - dózisnövelés (!) (jobban az ARB-vel, valószínűleg még jobban az Aliskerinnel tehető meg - RAS-blokkoló kombinálása más vérnyomás csökkentővel - kettő, esetleg három RAS-blokkoló kombinációja
 (jobban az ARB-vel, valószínűleg. még jobban az Aliskerinnel tehető meg. - RAS-blokkoló kombinálása más vérnyomás. csökkentővel. - kettő, esetleg három RAS-blokkoló kombinációja.")
12
RAAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás Új diabetes kialakulását csökkentik BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

14
RAAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás RAS-gátlók csökkentik új diabetes kialakulását BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

15
RAS-GÁTLÁS - BKH Vérnyomás csökkentésen túl csökkentik a BKH-t:
ACE-gátlók ARB-k Aliskerin

16
RAAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás RAS-k gátlők csökkentik új diabetes kialakulását BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

17
RAS-ATHEROSCLEROSIS AII fokozza az atherosclerosis progressióját:
- Weiss D et al Circulation 2001; 103: - Daugherty et al J Clin Invest 2000; 105: RAS-gátlók fékezik az atherosclerosis progressióját - Schiffrin ELet al Circulation 2000; 101: (losartan az endothelialis dysfunctio javításával) - Koh KK et al J Am Coll Cardiol 2003: 42: (az endothelialis függő vasomotor válasz javításával, a plasminogen activator inhibitor Type 1 csökkentésével) Th: Fokozott atherosclerosis jelei esetén - Anti.atherogen terápia mellett + RAS-gátlás v. RAS-gátlással kombinálás
 - Koh KK et al J Am Coll Cardiol 2003: 42: (az endothelialis függő vasomotor válasz javításával, a plasminogen. activator inhibitor Type 1 csökkentésével) Th: Fokozott atherosclerosis jelei esetén. - Anti.atherogen terápia mellett. + RAS-gátlás v. RAS-gátlással kombinálás.")
18
RAAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás Új diabetes kialakulását csökkentik BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

19
RAS-GÁTLÁS – PITVARFIBRILLATIO PREVENTIO
RAS-gátlással a pitvarfibrillatio jelentkezése csökkenthető: - Salehian O et al. Am Heart J 2007; 154:448-53 - Healy J ET AL. J Am Coll Cardiol 2005; ACE-gátlők: enalapril (SOLVD), lisinopril (Van Der Berg), trandolapril (TRACE) ARBk: irbesartan (MADRID), losartan(LIFE), valsartan (Val Heft)
, lisinopril (Van Der Berg), trandolapril (TRACE) ARBk: irbesartan (MADRID), losartan(LIFE), valsartan (Val Heft)")
20
RAAS-gátlás terápiás hatásai Vérnyomás csökkentésen túl
Antiproteinuriás Új diabetes kialakulását csökkentik BKH-t csökkentő Antiatherogen Pitvar-fibrillatio kialakulását védő Anti-tumor

21
Kaplan-Meier curves for incident and fatal cancer Each patient on ACEinhibitors (captopril, enalapril, lissinopril és mások) matched for age and sex with two patients on other antihypertensive drugs. p=0.02 for both comparisons. Note that scales on y axis differ. n összes= 5207 ACE gátlók= 3648 Többi szer= 1559 Lever AF et al. Lanecet 1998; 352: IV. Hámori Napok, Pécs

22
RAAS-GÁTLÓK HATÁSA MALIGNOMÁKBAN
Kedvező hatás: tüdő cc-ben vese cc-ben pancreas cc-ben melanomában leukemiában leiomyomában mamma cc-ban IV. Hámori Napok, Pécs

23
TUMOR ÉS RAAS GÁTLÁS Mind az ACE-gátlóknak, mind az ARB-knak van antitumor hatásuk, az ARB-k hatása erősebb A RAAS-gátlók az angiotensin-receptorok gátlásán keresztül fejtik ki fő tumor-genesist csökkentő hatásaikat: - antiproliferativ sejthatás - antiangiogenikus hatás Th.: Daganatok kezelésében kombinációs szerként jöhetnek szóba Az összefüggésben nincsenek kontrollált vizsgálatok IV. Hámori Napok, Pécs

24
A RAS-gátlás vérnyomás csökkentéstől független terápiás hatásai Következtetések
Antihypertensiv hatástól függetlenűl cardiovasculo-nephroprotectív hatású Bizonyos betegségekben, vagy hypertonia nélkül is előforduló kórállapotokban kedvező terápiás hatása van (tumor, pitvarfibrillatio, stb.) Ezek a kedvező terápiás hatások legalább részben az az AII antagonizálásán alapúlnak
 Ezek a kedvező terápiás hatások legalább részben az az AII antagonizálásán alapúlnak.")
25
Angiotensin II Plays a Central Role in Organ Damage
Atherosclerosis Stroke Atherosclerosis Abnormal coronary vasomotion Thrombosis MI Ang II AT1 afterload LVH* Fibrosis Ventricular Dilatation Heart Failure Death Angiotensin II Plays a Central Role in Organ Damage The deleterious effects of hypertension, oxidative stress, and Ang II extend beyond the heart, affecting multiple organ systems via hemodynamic and direct vascular/tissue effects1 Ang II has been implicated in cerebrovascular ischemia through the development of atherosclerosis2 Ang II is thought to deleteriously affect the coronary circulation by impairing normal coronary vasomotion, predisposing to atherosclerosis, and promoting thrombosis3-7 By inducing vasoconstriction and consequently increasing afterload, as well as contributing to left-ventricular hypertrophy, ventricular fibrosis, and ventricular afterload, Ang II contributes to the development of HF8,9 Although the exact pathophysiology remains unclear, Ang II is thought to contribute to renal failure by promoting intraglomerular hypertension, increased glomerular capillary permeability, interstitial fibrosis, and glomerulosclerosis10-12 glomerular capillary permeability Microcirculatory changes Glomerulosclerosis Renal Failure *LVH = left-ventricular hypertrophy. Willenheimer R, et al. Eur Heart J. 1999;20: ; Scheidegger KJ, Wood JM. J Vasc Res. 1997;34: ; Daugherty A et al. J Clin Invest. 2000;105: ; Hornig B et al. Circulation. 2001;103: ; Nickenig G, Harrison DG. Circulation. 2002;105: ; Sironi L et al. Hypertension. 2001;37: ; Oubina MP et al. J Hypertens. 2002;20: ; Jamali AH et al. Arch Intern Med. 2001;161: ; Dzau VJ. Arch Intern Med. 1993;153: ; Remuzzi G, Bertani T. N Engl J Med. 1998;339: ; Ruggenenti P et al. Lancet. 2001;357: ; Viberti G et al. Circulation. 2002;106:

26
Köszönöm a figyelmet!

28
DUAL RENIN-ANGIOTENSIN SYSTEM BLOCKADE IS HIGHLY EFFECTIVE TO IN NON-DIABETIC PROTEINURICS
9 non-diabetic renal patients (6 weeks treatment per dose) -25 Change of proteinuria (%) Losartan -50 -75 Lisinopril Combined -100 50 100 150 10 20 40 Laverman et al., Kidney Int, 2002
 -25. Change of proteinuria (%) Losartan Lisinopril. Combined Laverman et al., Kidney Int,")
29
COOPERATE Trial Profile
336 patients screened 35 excluded needed immediate dialysis no consent 301 took part in 18-week run-in 38 excluded dry cough angioedema skin rash 263 randomly allocated 89 losartan and placebo 86 trandolapril and placebo 88 losartan and trandolapril 3 lost in follow-up 1 moved away discontinuation 1 lost in follow-up (discontinuation) 3 lost in follow-up 1 protocol invalidation 2 discontinuation 86 could be analyzed for primary endpoint 85 could be analyzed for primary endpoint 85 could be analyzed for primary endpoint Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):
 3 lost in follow-up 1 protocol invalidation 2 discontinuation. 86 could be analyzed for primary endpoint. 85 could be analyzed for primary endpoint. 85 could be analyzed for primary endpoint. Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Lancet. 2003;361(9352):")
30
COOPERATE: Primary Endpoint
Doubling of Serum Creatinine or Progression to ESRD TrandolapriLosartan Losartan Tr Combination 30 25 20 Proportion Reaching Endpoint, % 15 10 5 P = 0.02 At the end of 3 years, 11% of patients receiving combination treatment reached the combined primary endpoint compared with 23% receiving trandolapril alone (P=0.018) and 23% receiving losartan alone (P=0.016). The combination was well tolerated, even in those patients with advanced renal insufficiency.1 1. Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Combination treatment of angiotensin-II receptor blocker and angiotensin-converting-enzyme inhibitor in non-diabetic renal disease (COOPERATE): a randomised controlled trial. Lancet. 2003;361:117–124. 5 12 18 24 30 36 Months After Randomization Number at Risk Losartan 89 88 84 79 65 59 47 Trandolapril 86 85 83 75 72 63 58 Combination 88 87 86 83 76 73 67 Reprinted with permission from Nakao N et al. Lancet. 2003;361:117–124.
 and 23% receiving losartan alone (P=0.016). The combination was well tolerated, even in those patients with advanced renal insufficiency Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T. Combination treatment of angiotensin-II receptor blocker and angiotensin-converting-enzyme inhibitor in non-diabetic renal disease (COOPERATE): a randomised controlled trial. Lancet. 2003;361:117– Months After Randomization. Number at Risk. Losartan Trandolapril Combination Reprinted with permission from Nakao N et al. Lancet. 2003;361:117–124.")
31
THE EFFECT OF LOSARTAN ON BLOOD PRESSURE AND URINARY PROTEIN EXCRETION
Gansevoort et al., Kidney Int, 1994

32
Clinical Trials and Renal Outcomes Based on Proteinuria Reduction
Progression of diabetic nephropathy/ESRD Protection No Protection Captopril Ramipril (AASK/REIN) Losartan (RENAAL) Irbesartan (IDNT) Amlodipine (IDNT) Amlodipine (AASK) Isradipine (STENO) Nifedipine Points of Emphasis/Key Messages This figure abstracts the outcomes of several clinical trials investigating the effects on renal health of therapeutic reduction of proteinuria indices. Probably the most important conclusion from these pooled data is that when proteinuria is reduced by 30-35%, there is a concomitant increase in time to dialysis. When there is NO reduction in proteinuria, there is also no change in the time to dialysis. Supporting Evidence This meta-analysis examined the relationship between therapeutic decreases in proteinuria in patients with type 2 diabetes and the length of independence from dialysis. In multiple studies, (eg, AASK, REIN, RENAAL and IDTN), progression of diabetic nephropathy and end-stage renal disease was curtailed by ACE inhibitors and angiotensin-receptor blockers. Conversely, 4 studies employing dihydropyridine calcium channel blockers (AASK, IDNT and STENO, and that by Abbott et al) showed no renoprotection conferred by amlodipine, isradipine or nifedipine. References Abbott K, Smith A, Bakris GL. Effects of dihydropyridine calcium antagonists on albuminuria in patients with diabetes. J Clin Pharmacol.1996;36: Brenner BM, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type-2 diabetes and nephropathy. N Engl J Med. 2001; 345(12): Lewis EJ, et al. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993; 329: Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type-2 diabetes. N Engl J Med. 2001; 345(12): Norgaard K, Jensen T, Christensen P, Feldt-Rasmussen B. A comparison of spirapril and isradipine in patients with diabetic nephropaty and hypertension. Blood Press. 1993;2(4): Wright JT, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease. JAMA. 2002:288(19); Ruggenenti P, Perna A, Gherardi G, et al. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria Lancet. 1999;354(9176): 30-35% proteinuria No proteinuria ESRD = End Stage Renal Disease Lewis EJ et al. N Engl J Med. 1993;329: ; Wright JT et al. JAMA. 2002; 288(19): ; Ruggenenti P et al. Lancet. 1999;354(9176): ; Brenner BM et al. N Engl J Med. 2001;345(12): ; Lewis EJ et al. N Engl J Med. 2001;345(12): ; Norgaard K et al. Blood Press.1993;2(4): ; Abbott K et al. J Clin Pharmacol. 1996;36;
 Losartan (RENAAL) Irbesartan (IDNT) Amlodipine (IDNT) Amlodipine (AASK) Isradipine (STENO) Nifedipine. Points of Emphasis/Key Messages. This figure abstracts the outcomes of several clinical trials investigating the effects on renal health of therapeutic reduction of proteinuria indices. Probably the most important conclusion from these pooled data is that when proteinuria is reduced by 30-35%, there is a concomitant increase in time to dialysis. When there is NO reduction in proteinuria, there is also no change in the time to dialysis. Supporting Evidence. This meta-analysis examined the relationship between therapeutic decreases in proteinuria in patients with type 2 diabetes and the length of independence from dialysis. In multiple studies, (eg, AASK, REIN, RENAAL and IDTN), progression of diabetic nephropathy and end-stage renal disease was curtailed by ACE inhibitors and angiotensin-receptor blockers. Conversely, 4 studies employing dihydropyridine calcium channel blockers (AASK, IDNT and STENO, and that by Abbott et al) showed no renoprotection conferred by amlodipine, isradipine or nifedipine. References. Abbott K, Smith A, Bakris GL. Effects of dihydropyridine calcium antagonists on albuminuria in patients with diabetes. J Clin Pharmacol.1996;36: Brenner BM, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type-2 diabetes and nephropathy. N Engl J Med. 2001; 345(12): Lewis EJ, et al. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993; 329: Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type-2 diabetes. N Engl J Med. 2001; 345(12): Norgaard K, Jensen T, Christensen P, Feldt-Rasmussen B. A comparison of spirapril and isradipine in patients with diabetic nephropaty and hypertension. Blood Press. 1993;2(4): Wright JT, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease. JAMA. 2002:288(19); Ruggenenti P, Perna A, Gherardi G, et al. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria Lancet. 1999;354(9176): % proteinuria. No proteinuria. ESRD = End Stage Renal Disease. Lewis EJ et al. N Engl J Med. 1993;329: ; Wright JT et al. JAMA. 2002; 288(19): ; Ruggenenti P et al. Lancet. 1999;354(9176): ; Brenner BM et al. N Engl J Med. 2001;345(12): ; Lewis EJ et al. N Engl J Med. 2001;345(12): ; Norgaard K et al. Blood Press.1993;2(4): ; Abbott K et al. J Clin Pharmacol. 1996;36;")
33
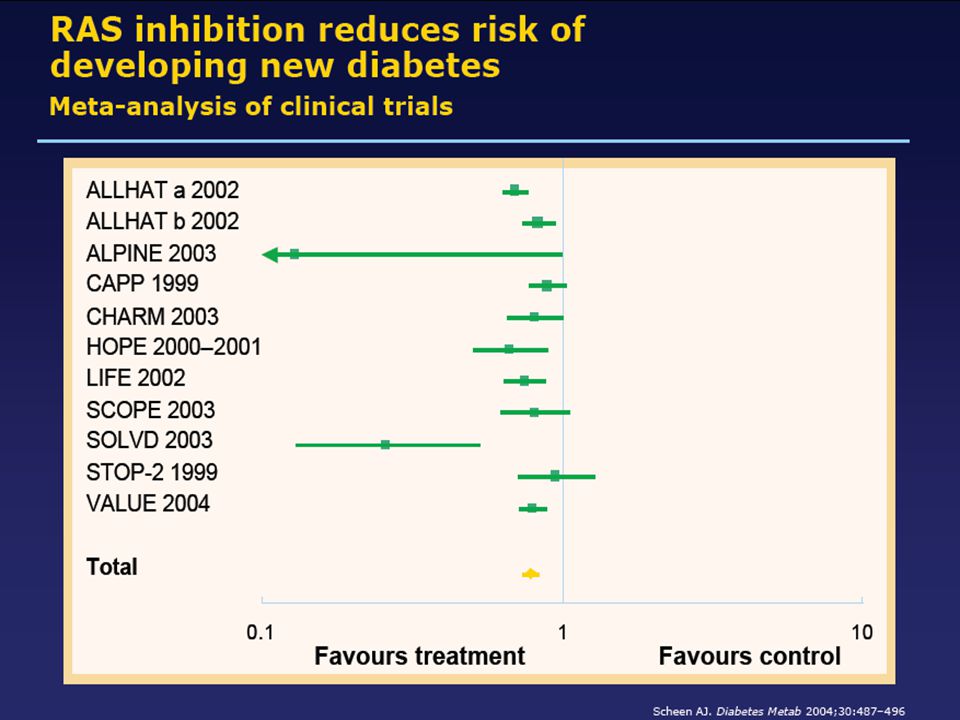
Relative Risk of New Onset Diabetes
Study Treatment 1 Increase in NOD Treatment 2 HOPE Placebo ± BB/diuretic 52% vs ACE-I ± BB/diuretic ALLHAT Diuretic 43% vs ACE-I INSIGHT Diuretic ± BB vs DHP-CCB LIFE BB + diuretic 32% vs ARB VALUE DHP-CCB-based 25% vs ARB-based 18% INVEST BB-based + diuretic 17% vs NDHP-CCB-based CHARM vs ARB ± BB/diuretic CAPPP Diuretics, BB 13% Points of Emphasis/Key Messages In a review of 8 landmark clinical trials including over 194,585 patients, diuretics and/or β-blockers were consistently associated with an increased incidence of new-onset diabetes (NOD). As shown in the HOPE study, addition of an ACE-I to a β-blocker plus diuretic combination effectively halved the incidence of NOD. Treatments based on CCBs and/or ACEs/ARBs consistently result in lower incidences of NOD. Supporting Evidence HOPE – 9297 high-risk patients, 55 years of age with evidence of CVD and 1 other CVD risk factor assigned to receive ramipril 10 mg daily or placebo for a mean of 5 years. Significantly fewer patients in the ramipril group developed a new diagnosis of diabetes (102 vs 155; RR, 0.66, P < .001). ALLHAT – 33,357 patients aged 55 years with hypertension and at least 1 other CHD risk factor were randomly assigned to receive chlortalidone, 12.5 to 25 mg/d (n = 15,255); amlodipine, 2.5 to 10 mg/d (n = 9048); or lisinopril, 10 to 40 mg/d (n = 9054) for planned follow-up of approximately 4 to 8 years. The rates of new-onset diabetes were 11.6%, 9.8% and 8.1% respectively (P < .001). The differential in rates between the diuretic vs ACE-I group was 43% (11.6/8), and that between the diuretic and the CCB was 18% (11.6/9.8). INSIGHT – A prospective, randomized, double-blind trial in 6331 patients aged years with HTN and at least 1 additional risk factor. Patients were randomly assigned nifedipine GITS 30 mg (n = 3157) or co-amilozide 25/2.5 (n = 3164). Dose titration was by dose doubling and addition of atenolol mg or enalapril 5-10 mg. Follow-up was over approximately 3-5 years. The co-amilozide group developed new diabetes at a rate of 4.3% vs 3.0% for those on nifedipine P = .01. LIFE – 89,193 patients aged years (mean age 67 years) with hypertension and documented LVH were randomly assigned to once-daily losartan-or atenolol-based treatment and followed for at least 4 years (mean 4.8 years). [Lindholm/1879/C1/P2/L1] Treatment with losartan was associated with lower risk of development of diabetes within each of the 4 quartiles of the risk score. NOD occurred in 242 patients receiving losartan and 320 receiving atenolol. (Continued on following slide) References The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril on cardiovascular events in high-risk patients. N Engl J Med. 2000;342: The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major Outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. JAMA. 2003;288: Brown MJ, Palmer CR, Casraine A, et al. Morbidity and mortality in patients randomized to double-blind treatment with a long-acting calcium channel blocker or diuretic in the International Nifedipine study: Intervention as a Goal in Hypertension Treatment (INSIGHT) Lancet. 2000;356: NOD = New-onset diabetes; BB = beta-blocker Lancet. 1999;353: ; Lancet. 2003;362: ; JAMA. 2003;290: ; Lancet. 2000;356: ; Lancet 2004;363: ; JAMA. 2002;288: ; N Engl J Med. 2000;342: ; J Hypertension. 2002;20: ; Am J Hypertens. 2003;16:
. As shown in the HOPE study, addition of an ACE-I to a β-blocker plus diuretic combination effectively halved the incidence of NOD. Treatments based on CCBs and/or ACEs/ARBs consistently result in lower incidences of NOD. Supporting Evidence. HOPE – 9297 high-risk patients, 55 years of age with evidence of CVD and 1 other CVD risk factor assigned to receive ramipril 10 mg daily or placebo for a mean of 5 years. Significantly fewer patients in the ramipril group developed a new diagnosis of diabetes (102 vs 155; RR, 0.66, P < .001). ALLHAT – 33,357 patients aged 55 years with hypertension and at least 1 other CHD risk factor were randomly assigned to receive chlortalidone, 12.5 to 25 mg/d (n = 15,255); amlodipine, 2.5 to 10 mg/d (n = 9048); or lisinopril, 10 to 40 mg/d (n = 9054) for planned follow-up of approximately 4 to 8 years. The rates of new-onset diabetes were 11.6%, 9.8% and 8.1% respectively (P < .001). The differential in rates between the diuretic vs ACE-I group was 43% (11.6/8), and that between the diuretic and the CCB was 18% (11.6/9.8). INSIGHT – A prospective, randomized, double-blind trial in 6331 patients aged years with HTN and at least 1 additional risk factor. Patients were randomly assigned nifedipine GITS 30 mg (n = 3157) or co-amilozide 25/2.5 (n = 3164). Dose titration was by dose doubling and addition of atenolol mg or enalapril 5-10 mg. Follow-up was over approximately 3-5 years. The co-amilozide group developed new diabetes at a rate of 4.3% vs 3.0% for those on nifedipine P = .01. LIFE – 89,193 patients aged years (mean age 67 years) with hypertension and documented LVH were randomly assigned to once-daily losartan-or atenolol-based treatment and followed for at least 4 years (mean 4.8 years). [Lindholm/1879/C1/P2/L1] Treatment with losartan was associated with lower risk of development of diabetes within each of the 4 quartiles of the risk score. NOD occurred in 242 patients receiving losartan and 320 receiving atenolol. (Continued on following slide) References. The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril on cardiovascular events in high-risk patients. N Engl J Med. 2000;342: The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major Outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. JAMA. 2003;288: Brown MJ, Palmer CR, Casraine A, et al. Morbidity and mortality in patients randomized to double-blind treatment with a long-acting calcium channel blocker or diuretic in the International Nifedipine study: Intervention as a Goal in Hypertension Treatment (INSIGHT) Lancet. 2000;356: NOD = New-onset diabetes; BB = beta-blocker. Lancet. 1999;353: ; Lancet. 2003;362: ; JAMA. 2003;290: ; Lancet. 2000;356: ; Lancet 2004;363: ; JAMA. 2002;288: ; N Engl J Med. 2000;342: ; J Hypertension. 2002;20: ; Am J Hypertens. 2003;16:")
34
Clinical Trials and Renal Outcomes Based on Proteinuria Reduction
Progression of diabetic nephropathy/ESRD Protection No Protection Captopril Ramipril (AASK/REIN) Losartan (RENAAL) Irbesartan (IDNT) Amlodipine (IDNT) Amlodipine (AASK) Isradipine (STENO) Nifedipine Points of Emphasis/Key Messages This figure abstracts the outcomes of several clinical trials investigating the effects on renal health of therapeutic reduction of proteinuria indices. Probably the most important conclusion from these pooled data is that when proteinuria is reduced by 30-35%, there is a concomitant increase in time to dialysis. When there is NO reduction in proteinuria, there is also no change in the time to dialysis. Supporting Evidence This meta-analysis examined the relationship between therapeutic decreases in proteinuria in patients with type 2 diabetes and the length of independence from dialysis. In multiple studies, (eg, AASK, REIN, RENAAL and IDTN), progression of diabetic nephropathy and end-stage renal disease was curtailed by ACE inhibitors and angiotensin-receptor blockers. Conversely, 4 studies employing dihydropyridine calcium channel blockers (AASK, IDNT and STENO, and that by Abbott et al) showed no renoprotection conferred by amlodipine, isradipine or nifedipine. References Abbott K, Smith A, Bakris GL. Effects of dihydropyridine calcium antagonists on albuminuria in patients with diabetes. J Clin Pharmacol.1996;36: Brenner BM, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type-2 diabetes and nephropathy. N Engl J Med. 2001; 345(12): Lewis EJ, et al. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993; 329: Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type-2 diabetes. N Engl J Med. 2001; 345(12): Norgaard K, Jensen T, Christensen P, Feldt-Rasmussen B. A comparison of spirapril and isradipine in patients with diabetic nephropaty and hypertension. Blood Press. 1993;2(4): Wright JT, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease. JAMA. 2002:288(19); Ruggenenti P, Perna A, Gherardi G, et al. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria Lancet. 1999;354(9176): 30-35% proteinuria No proteinuria ESRD = End Stage Renal Disease Lewis EJ et al. N Engl J Med. 1993;329: ; Wright JT et al. JAMA. 2002; 288(19): ; Ruggenenti P et al. Lancet. 1999;354(9176): ; Brenner BM et al. N Engl J Med. 2001;345(12): ; Lewis EJ et al. N Engl J Med. 2001;345(12): ; Norgaard K et al. Blood Press.1993;2(4): ; Abbott K et al. J Clin Pharmacol. 1996;36;
 Losartan (RENAAL) Irbesartan (IDNT) Amlodipine (IDNT) Amlodipine (AASK) Isradipine (STENO) Nifedipine. Points of Emphasis/Key Messages. This figure abstracts the outcomes of several clinical trials investigating the effects on renal health of therapeutic reduction of proteinuria indices. Probably the most important conclusion from these pooled data is that when proteinuria is reduced by 30-35%, there is a concomitant increase in time to dialysis. When there is NO reduction in proteinuria, there is also no change in the time to dialysis. Supporting Evidence. This meta-analysis examined the relationship between therapeutic decreases in proteinuria in patients with type 2 diabetes and the length of independence from dialysis. In multiple studies, (eg, AASK, REIN, RENAAL and IDTN), progression of diabetic nephropathy and end-stage renal disease was curtailed by ACE inhibitors and angiotensin-receptor blockers. Conversely, 4 studies employing dihydropyridine calcium channel blockers (AASK, IDNT and STENO, and that by Abbott et al) showed no renoprotection conferred by amlodipine, isradipine or nifedipine. References. Abbott K, Smith A, Bakris GL. Effects of dihydropyridine calcium antagonists on albuminuria in patients with diabetes. J Clin Pharmacol.1996;36: Brenner BM, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type-2 diabetes and nephropathy. N Engl J Med. 2001; 345(12): Lewis EJ, et al. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med. 1993; 329: Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type-2 diabetes. N Engl J Med. 2001; 345(12): Norgaard K, Jensen T, Christensen P, Feldt-Rasmussen B. A comparison of spirapril and isradipine in patients with diabetic nephropaty and hypertension. Blood Press. 1993;2(4): Wright JT, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease. JAMA. 2002:288(19); Ruggenenti P, Perna A, Gherardi G, et al. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria Lancet. 1999;354(9176): % proteinuria. No proteinuria. ESRD = End Stage Renal Disease. Lewis EJ et al. N Engl J Med. 1993;329: ; Wright JT et al. JAMA. 2002; 288(19): ; Ruggenenti P et al. Lancet. 1999;354(9176): ; Brenner BM et al. N Engl J Med. 2001;345(12): ; Lewis EJ et al. N Engl J Med. 2001;345(12): ; Norgaard K et al. Blood Press.1993;2(4): ; Abbott K et al. J Clin Pharmacol. 1996;36;")
35
ARB DECREASES THE ATHEROSCLEROTIC PROCESSES
Compared with placebo, candesartan therapy significantly lowered plasma levels of plasminogen activator inhibitor type-1 (PAI-1) from the respective baseline levels (p < 0.001). Open circles = mean values.
 from the respective baseline levels (p < 0.001). Open circles = mean values.")
Hasonló előadás













 MORE?” symposium Washington.>")






