Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
A hagyományos kardiovaszkuláris rizikófaktorok és a diabetes
microvascularis szövődményeinek összefüggése Prof. Dr. Kempler Péter egyetemi tanár Semmelweis Egyetem I. sz. Belgyógyászati Klinika, Budapest

2
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC7 Report. JAMA 2003; 289: Hypertension† Cigarette smoking Obesity (BMI ≥ 30) † Physical inactivity Dyslipidaemia † Diabetes mellitus † Microalbuminuria or estimated GFR < 60 ml/min Age (> 55 years for men, > 65 years for women) Family history of premature cardiovascular disease (men < 55 years, women < 65 years)
 † Physical inactivity. Dyslipidaemia † Diabetes mellitus † Microalbuminuria or estimated GFR < 60 ml/min. Age (> 55 years for men, > 65 years for women) Family history of premature cardiovascular disease. (men < 55 years, women < 65 years)")
3
Risk of CHD Death According to SBP and DBP in MRFIT
4 Systolic blood pressure (SBP) Diastolic blood pressure (DBP) 3 Relative risk of CHD mortality 2 1 Risk of CHD Death According to SBP and DBP in MRFIT With some 350,000 men screened from 1973 to 1975 and followed for major fatal outcomes, the Multiple Risk Factor Intervention Trial (MRFIT) has an enormously powerful database and permits a close look at the relationship of systolic blood pressure (SBP) and diastolic blood pressure (DBP), independently, to coronary heart disease (CHD) mortality risk. During 11.6 years of follow-up, there were 7,150 deaths due to CHD. Compared with subjects in the bottom decile of blood pressure (SBP <112; DBP <71), those at the top decile of the blood pressure distribution (SBP 151; DBP 98) were at markedly increased risk for death from CHD. The relationship of rising blood pressure to risk was continuous and graded, and was steeper for SBP compared with DBP. The average blood pressure levels of the MRFIT cohort were SBP 130 mmHg and DBP 84 mmHg. Optimal SBP, the level with the lowest death rate, was <120 mmHg. Statistical significance between SBP and CHD, and DBP and CHD. SBP: 3rd decile, P<0.05; 4th through 10th deciles, P<0.001. DBP: 4th decile, P<0.01; 5th through 10th deciles, P<0.001. Reference: He J, Whelton PK. Elevated systolic blood pressure and risk of cardiovascular and renal disease: overview of evidence from observational epidemiologic studies and randomized controlled trials. Am Heart J 1999; 138 (3 Pt 2):211-9. Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. US population data. Arch Intern Med 1993; 153 (5): Decile 1 2 3 4 5 6 7 8 9 10 (lowest 10%) (highest 10%) <112 <71 >151 >98 SBP (mmHg) DBP (mmHg) CHD=coronary heart disease He J, et at. Am Heart J. 1999;138:
 Diastolic blood pressure (DBP) 3. Relative risk of. CHD mortality Risk of CHD Death According to SBP and DBP in MRFIT. With some 350,000 men screened from 1973 to 1975 and followed for major fatal outcomes, the Multiple Risk Factor Intervention Trial (MRFIT) has an enormously powerful database and permits a close look at the relationship of systolic blood pressure (SBP) and diastolic blood pressure (DBP), independently, to coronary heart disease (CHD) mortality risk. During 11.6 years of follow-up, there were 7,150 deaths due to CHD. Compared with subjects in the bottom decile of blood pressure (SBP <112; DBP <71), those at the top decile of the blood pressure distribution (SBP 151; DBP 98) were at markedly increased risk for death from CHD. The relationship of rising blood pressure to risk was continuous and graded, and was steeper for SBP compared with DBP. The average blood pressure levels of the MRFIT cohort were SBP 130 mmHg and DBP 84 mmHg. Optimal SBP, the level with the lowest death rate, was <120 mmHg. Statistical significance between SBP and CHD, and DBP and CHD. SBP: 3rd decile, P<0.05; 4th through 10th deciles, P< DBP: 4th decile, P<0.01; 5th through 10th deciles, P< Reference: He J, Whelton PK. Elevated systolic blood pressure and risk of cardiovascular and renal disease: overview of evidence from observational epidemiologic studies and randomized controlled trials. Am Heart J 1999; 138 (3 Pt 2): Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. US population data. Arch Intern Med 1993; 153 (5): Decile (lowest 10%) (highest 10%) <112 < >151 >98. SBP (mmHg) DBP (mmHg) CHD=coronary heart disease. He J, et at. Am Heart J. 1999;138:")
4
Cholesterol and triglyceride as risk factors of coronary heart disease
mmol \ lit. CHD cases ( per 1000 ) Cholesterol mmol \ lit. PROCAM ( 6 years )
 Cholesterol. mmol \ lit. PROCAM ( 6 years )")
6
Atherosclerosis risk factors and the CVD mortality
among men with and without diabetes (Diabetes Care, 1993, 16, ) CVD death/men/year DM- DM+
 CVD death/men/year. DM- DM")
7
Howard BV. et al. Coronary Heart Disease Risk Equivalence in Diabetes Depends on Concomitant Risk Factors. Diabetes Care 29: , 2006. The 10-year cumulative incidence of CHD by numbers of risk factors (men and women combined).
.")
8
Kockázatbecslő táblázat
Fatális szív- és érrendszeri események előfordulási gyakorisága 10 éven belül Nem dohányzó Férfi Dohányzó 10-14% >15% 5-9% 3-4% 2% <1% 1% 4 5 6 7 8 4 5 8 7 6 180 160 140 120 65 éves 180 160 140 120 180 160 140 120 60 éves 180 160 140 120 180 160 140 120 55 éves 180 160 140 120 Szisztolés vérnyomás (Hgmm) 180 160 140 120 50 éves 180 160 140 120 180 160 140 120 40 éves 180 160 140 120
 éves éves")
9
Type 2 diabetes is NOT a mild disease
Stroke Diabetic retinopathy 1.2- to 1.8-fold increase in stroke3 Leading cause of blindness in working-age adults1 Cardiovascular disease 75% diabetic patients die from CV events4 Diabetic nephropathy Diabetic neuropathy Leading cause of end-stage renal disease2 Leading cause of non-traumatic lower extremity amputations5 1Fong DS, et al. Diabetes Care 2003; 26 (Suppl. 1):S99–S102. 2Molitch ME, et al. Diabetes Care 2003; 26 (Suppl. 1):S94–S98. 3Kannel WB, et al. Am Heart J 1990; 120:672–676. 4Gray RP & Yudkin JS. In Textbook of Diabetes 1997. 5Mayfield JA, et al. Diabetes Care 2003; 26 (Suppl. 1):S78–S79.
:S99–S102. 2Molitch ME, et al. Diabetes Care 2003; 26 (Suppl. 1):S94–S98. 3Kannel WB, et al. Am Heart J 1990; 120:672–676. 4Gray RP & Yudkin JS. In Textbook of Diabetes Mayfield JA, et al. Diabetes Care 2003; 26 (Suppl. 1):S78–S79.")
10
Type 2 diabetes – the microvascular burden is already present at diagnosis
21% Retinopathy1 Nephropathy2 18% 20% Erectile dysfunction1 Complications start early in the development of Type 2 diabetes CORE SLIDE Increasing blood glucose levels are associated with an increased risk of several debilitating microvascular complications.1-3 People with diabetes are at least 15 times more likely to undergo lower limb amputation than the general population.4,5 More than 50% of patients with Type 2 diabetes have complications at diagnosis and this figure rises to 70% if hypertension and impotence are included.1 Patients with Type 2 diabetes are also at greatly increased risk of cardiovascular disease.6 Link to next slide: How do complications occur? References 1. UKPDS Group. Diabetes Res 1990; 13: 1–11. 2. The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317. 3. Stratton IM et al. BMJ 2000; 321: 405–412. 4. King’s Fund. Counting the cost. The real impact of non insulin dependent diabetes. London: British Diabetic Association, 1996. 5. Most RS et al. Diabetes Care 1983; 6: 87–91. 6. Stamler J et al. Diabetes Care 1993; 16: 434–444. 12% Neuropathy1 1. UKPDS Group. Diabetes Res 1990; 13: 1– The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317.

11
Jarrett RJ. et al. Microalbuminuria predicts mortality in non-insulin-dependent diabetes.
Diabetic Med 1; 17-19, 1984. Mogensen CE.: Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. N Engl J Med 310; , 1984.

12
Mykkänen L. et al. Microalbuminuria precedes the development of NIDDM.
Diabetes 1994; 43:

13
Yudkin JS, Forest RO, Jackson CA.
Microalbuminuria as a predictor of vascular disease in non-diabetic subjects. Lancet 1988; II:

14
Cardiovascular morbidity and mortality
Astrup, AS. et al. Cardiac Autonomic Neuropathy Predicts Cardiovascular Morbidity and Mortality in Type 1 Diabetic Patients With Diabetic Nephropathy Diabetes Care 2006; 29: Cardiovascular morbidity and mortality Nephropathy Normoalbuminuria Normal HRV borderline normal HRV abnormal HRV

15
EURODIAB IDDM Complications Study
Risk Factors for Progression to Microalbuminuria (Univariate Analysis) HbA1c, AER Fasting Triglyceride, HDL-C, LDL-C BMI, WHR Presence of Retinopathy/Neuropathy NOT Systolic BP, Diastolic BP, Smoking Chaturvedi et al, Kidney International 2001;60:
 HbA1c, AER. Fasting Triglyceride, HDL-C, LDL-C. BMI, WHR. Presence of Retinopathy/Neuropathy. NOT Systolic BP, Diastolic BP, Smoking. Chaturvedi et al, Kidney International 2001;60:")
16
EURODIAB IDDM Complications Study
Risk Factors for Progression to Microalbuminuria Adjusted for Duration, HbA1c and AER Progressors Non-progressors P Mean Fasting Triglyceride (mmol/L) HDL-C (mmol/L) LDL-C (mmol/L) BMI (Kg/m2) WHR Relative Risk of Progression - Any Retinopathy Chaturvedi et al, Kidney International 2001;60:
 HDL-C (mmol/L) LDL-C (mmol/L) BMI (Kg/m2) WHR Relative Risk of Progression. - Any Retinopathy Chaturvedi et al, Kidney International 2001;60:")
17
EURODIAB IDDM Complications Study
Standardised Estimates of Relative Risk (SERR) for Incidence of Complications NEPHROPATHY AGE/DURATION* - HbA1c 1.57 ( ) AER 1.45 ( ) TRIGLYCERIDE 1.31 ( ) WHR 1.27 ( ) BMI - RETINOPATHY 1.32 ( )* 1.93 ( ) - 1.42 ( ) 1.32 ( ) NEUROPATHY 1.39 ( ) 1.20 ( ) - 1.33 ( ) 1.39 ( ) Insulin Resistance?
 for Incidence of Complications. NEPHROPATHY. AGE/DURATION* - HbA1c 1.57 ( ) AER 1.45 ( ) TRIGLYCERIDE 1.31 ( ) WHR 1.27 ( ) BMI - RETINOPATHY ( )* 1.93 ( ) ( ) 1.32 ( ) NEUROPATHY ( ) 1.20 ( ) ( ) 1.39 ( ) Insulin Resistance")
18
Giorgino et al. Factors associated with progression to macroalbuminuria in microalbuminuric Type 1 diabetic patients: The EURODIAB Prospective Complications Study. Diabetologia 2004; 47: Factors associated with progression to macroalbuminuria higher AER values sub-optimal metabolic control excess body fat peripheral neuropathy

19
Hadjadj et al. Different patterns of insulin resistance in relatives of Type 1 diabetic patients with retinopathy and nephropathy. Diabetes Care 2004; 27: Familial insulin resistance segregates with diabetic complications Lipid disorders and obesity segregate with diabetic nephropathy Arterial hypertension and obesity segregate with diabetic retinopathy

20
Type 2 diabetes – the microvascular burden is already present at diagnosis
21% Retinopathy1 Nephropathy2 18% 20% Erectile dysfunction1 Complications start early in the development of Type 2 diabetes CORE SLIDE Increasing blood glucose levels are associated with an increased risk of several debilitating microvascular complications.1-3 People with diabetes are at least 15 times more likely to undergo lower limb amputation than the general population.4,5 More than 50% of patients with Type 2 diabetes have complications at diagnosis and this figure rises to 70% if hypertension and impotence are included.1 Patients with Type 2 diabetes are also at greatly increased risk of cardiovascular disease.6 Link to next slide: How do complications occur? References 1. UKPDS Group. Diabetes Res 1990; 13: 1–11. 2. The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317. 3. Stratton IM et al. BMJ 2000; 321: 405–412. 4. King’s Fund. Counting the cost. The real impact of non insulin dependent diabetes. London: British Diabetic Association, 1996. 5. Most RS et al. Diabetes Care 1983; 6: 87–91. 6. Stamler J et al. Diabetes Care 1993; 16: 434–444. 12% Neuropathy1 1. UKPDS Group. Diabetes Res 1990; 13: 1– The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317.

21
Retinopathia diabetica
A fejlett ipari országokban a munkaképes korúak körében a vakság leggyakoribb oka cukorbetegekben Vakság 25x gyakrabban alakul ki, mint nem diabetesesekben A diabetes gondozás leghatékonyabb része a retinopathia szűrése Diabetesesekben a cataracta 1,6x a glaucoma 1,4x gyakoribb, mint cukorbetegségben nem szenvedőkben

22
Chaturvedi N et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in Type 1 diabetes. The EURODIAB Prospective Complications Study.Diabetes Care 2001; 24: Retinopathy incidence during 7,3 year follow-up was 56% Key risk factors: - diabetes duration - glycemic control – no evidence of a threshold effect for HbA1c

23
Chaturvedi N et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in Type 1 diabetes. The EURODIAB Prospective Complications Study. Diabetes Care 2001; 24: Risk factors for the incidence of retinopathy – univariate analysis: Duration of diabetes p = 0,0002 HbA1c p = 0,0001 AER (μg/min) p = 0,001 Cholesterol p = 0,008 Fasting triglyceride p = 0,0001
 p = 0,001. Cholesterol p = 0,008. Fasting triglyceride p = 0,0001.")
24
Chaturvedi N et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in Type 1 diabetes. The EURODIAB Prospective Complications Study. Diabetes Care 2001; 24: Risk factors for the incidence of retinopathy – univariate analysis: Fibrinogen p = 0,05 von Willebrand factor p = 0,04 γGT p = 0,02 Waist – hip ratio p = 0,0001 Insulin dose/weight p = 0,003

25
Chaturvedi N et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in Type 1 diabetes. The EURODIAB Prospective Complications Study. Diabetes Care 2001; 24: No associations were observed for cardiovascular disease, smoking, or blood pressure: mean blood pressures were relatively low at baseline in the study blood presssure was one of the few key risk factors measured locally

26
Chaturvedi N et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in Type 1 diabetes. The EURODIAB Prospective Complications Study. Diabetes Care 2001; 24: Standardized regression estimates Risk factor SRE (95% CI) P Duration 1,32 (1,07-1,61) 0,008 HbA1c 1,93 (1,52-2,44) 0,0001 Fasting triglyceride* 1,24 (1,01-1,54) 0,04 Waist-to-hip ratio 1,32 (1,07-1,63) 0,01 * Analysis performed on log-transformed variables
 P. Duration 1,32 (1,07-1,61) 0,008. HbA1c 1,93 (1,52-2,44) 0,0001. Fasting triglyceride* 1,24 (1,01-1,54) 0,04. Waist-to-hip ratio 1,32 (1,07-1,63) 0,01. * Analysis performed on log-transformed variables.")
27
Az autonom neuropathia prognózisa diabetes mellitusban
Követési idő: 5,8 év (metaanalízis) Autonom neuropathia – + Ziegler D. Diabetes Metab Rev 1994; 10:
 Autonom neuropathia. – + Ziegler D. Diabetes Metab Rev 1994; 10:")
28
Silent myocardialis infarctus
Balkamra-elégtelenség, tüdőoedema Ketoacidozis Hányás Collapsus hátterében cukorbetegekben mindig gondolni kell infarctus lehetőségére is.

29
A cardialis autonom neuropathia (CAN) és a néma („silent”) myocardialis infarctus közötti összefüggés 1,96 (1,53-2,51) összesített adatok, n=1468 p<0,001 DIAD n=1123 CAN = az ISzB erős előrejelzője Vinik et al., Diabetes Care 26: , 2003 Wackers et al Diabetes Care 27; , 2005 Logaritmikus prevalencia arány
 összesített adatok, n=1468 p<0,001. DIAD n=1123 CAN = az ISzB erős előrejelzője Vinik et al., Diabetes Care 26: , Wackers et al Diabetes Care 27; , Logaritmikus prevalencia arány.")
30
Hónapok óta fennálló tünetmentes talpi fekély
Zick R., Brockhaus KE. Diabetes mellitus. Fußfibel, Kirchheim, Mainz 2000.

31
Etiology of foot ulcers
Purely ischaemic Neuropathic or neuroischaemic Boulton AJM. Lowering the risk of neuropathy, foot ulcers and amputation. Diabetic Med 1998; 15 (Suppl 4):
:")
32
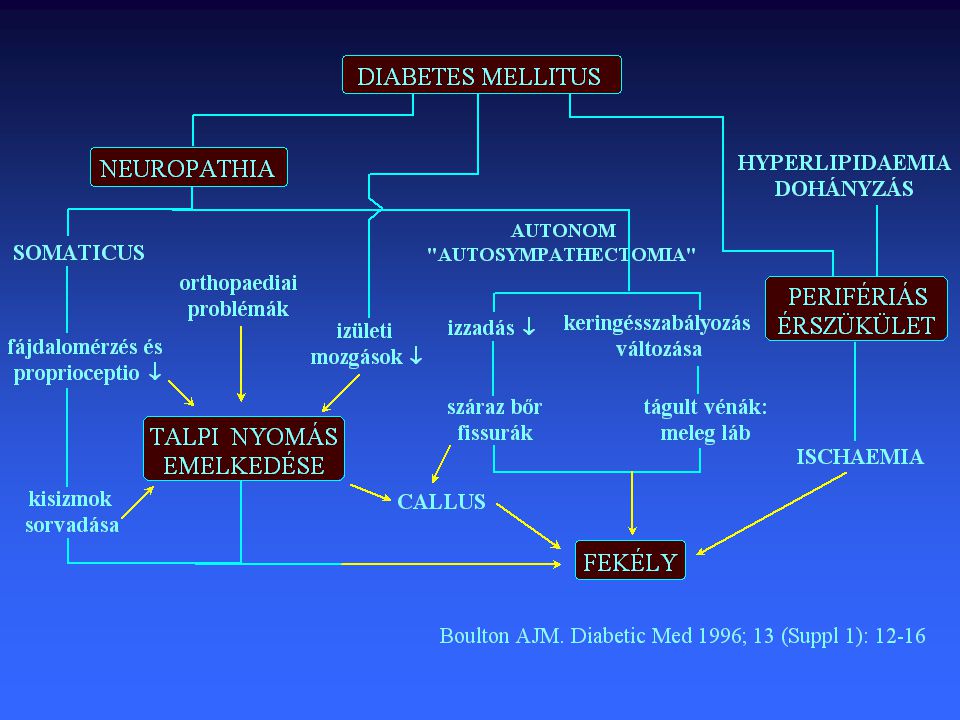
gyakoribb infekciók rosszabb sebgyógyulás
Sensoros neuropathia hypaesthesia trauma, microtrauma microangio-pathia Trophicus ulcus gyakoribb infekciók rosszabb sebgyógyulás Gangraena

33
Esetismertetés 32 éves diabeteses férfi Diabetes tartam: 20 év
HbA1C: 6,7% Súlyos sensoros neuropathia, orvosa tanácsa ellenére 20km-t futott Zick R., Brockhaus KE. Diabetes mellitus. Fußfibel, Kirchheim, Mainz 2000.

34
Lábsérülések 20km futást követően súlyos sensoros neuropathia fennállása esetén
Zick R., Brockhaus KE. Diabetes mellitus. Fußfibel, Kirchheim, Mainz 2000.

36
A diabeteses láb klinikai stádiumai
Meggitt BF. Diabetes. In: Helal B et al. (eds). The Foot pp
. The Foot pp")
37
Alsó végtagi amputációk aránya cukor-betegekben a nem-diabetesesekhez viszonyítva
30,0 x (Most és mtsai. Diabetes Care 1983;6: 87-91) 37,5 x (Dánia,1988) 11,7 x (ADA, 1992) 17,0 x (Humphrey és mtsai. Arch Intern Med ;154: ) 45,0 x (Standl és mtsai. Diab Stoffw 1996;5: 29-32)
 37,5 x (Dánia,1988) 11,7 x (ADA, 1992) 17,0 x (Humphrey és mtsai. Arch Intern Med 1994;154: ) 45,0 x (Standl és mtsai. Diab Stoffw 1996;5: 29-32)")
39
Lábamputációk cukorbetegekben - 2005
Cukorbetegek kórházi felvételére a fejlett országokban a leggyakrabban lábszövődmények miatt kerül sor A legtöbb amputációt talpi fekély előzi meg Napjainkban a diabetesesekben történt alsó végtagi amputációk 85%-át tartják megelőzhetőnek. IDF, 2005

41
Nem traumás eredetű alsó végtagi amputációk felét cukorbetegekben végzik
Magyarországon évente cukorbeteg lábát amputálják. Neuropathiás eredetű amputációnak nem szabadna előfordulnia.

42
Charcot - osteoarthropathia
Zick R., Brockhaus KE. Diabetes mellitus. Fußfibel, Kirchheim, Mainz 2000.

43
Type 2 diabetes – the microvascular burden is already present at diagnosis
21% Retinopathy1 Nephropathy2 18% 20% Erectile dysfunction1 Complications start early in the development of Type 2 diabetes CORE SLIDE Increasing blood glucose levels are associated with an increased risk of several debilitating microvascular complications.1-3 People with diabetes are at least 15 times more likely to undergo lower limb amputation than the general population.4,5 More than 50% of patients with Type 2 diabetes have complications at diagnosis and this figure rises to 70% if hypertension and impotence are included.1 Patients with Type 2 diabetes are also at greatly increased risk of cardiovascular disease.6 Link to next slide: How do complications occur? References 1. UKPDS Group. Diabetes Res 1990; 13: 1–11. 2. The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317. 3. Stratton IM et al. BMJ 2000; 321: 405–412. 4. King’s Fund. Counting the cost. The real impact of non insulin dependent diabetes. London: British Diabetic Association, 1996. 5. Most RS et al. Diabetes Care 1983; 6: 87–91. 6. Stamler J et al. Diabetes Care 1993; 16: 434–444. 12% Neuropathy1 1. UKPDS Group. Diabetes Res 1990; 13: 1– The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317.

44
Tesfaye et al. Prevalence of diabetic peripheral neuropathy and its relation to glycaemic control and potential risk factors: the EURODIAB IDDM Complications Study. Diabetologia 1996; Significant correlations were observed between the presence of diabetic peripheral neuropathy with age duration of diabetes (p<0,05) quality of metabolic control (p<0,001) confirming previous associations.
 quality of metabolic control (p<0,001) confirming previous associations.")
45
Tesfaye et al. Prevalence of diabetic peripheral neuropahy and its relation to glycaemic control and potential risk factors: the EURODIAB IDDM Complications Study. Diabetologia 1996; Significant correlations were observed between the presence of diabetic peripheral neuropathy with height (p<0,01) the presence of backround of proliferative retinopathy (p<0,01) cigarette smoking (p<0,001) HDL-cholesterol (p<0,001) presence of cardiovascular disease (p<0,05) confirming previous associations.
 the presence of backround of proliferative retinopathy (p<0,01) cigarette smoking (p<0,001) HDL-cholesterol (p<0,001) presence of cardiovascular disease (p<0,05) confirming previous associations.")
46
Tesfaye et al. Prevalence of diabetic peripheral neuropahy and its relation to glycaemic control and potential risk factors: the EURODIAB IDDM Complications Study. Diabetologia 1996; Significant correlations were observed between the presence of diabetic peripheral neuropathy with diastolic blood pressure (p<0,05) presence of severe ketoacidosis (p<0,01) fasting triglyceride (p<0,001) presence of microalbuminuria (p<0,01) identifying new associations.
 presence of severe ketoacidosis (p<0,01) fasting triglyceride (p<0,001) presence of microalbuminuria (p<0,01) identifying new associations.")
47
relative risk of abnormal R-R ratio (p-value, testing for trend)
Kempler P, Tesfaye S, Chaturvedi N. et al. Autonomic neuropathy is associated with increased cardiovascular risk factors: the EURODIAB IDDM Complications Study. Diabetic Med 2002; 19: * adjusted for age, duration and HbA1C ** testing difference from non-smoking Crude Adjusted* relative risk of abnormal R-R ratio (p-value, testing for trend) Smoking - ex - current p < 0,01** p < 0,0001** p < 0,05** Blood pressure - systolic - diastolic p < 0,05 N.S. Total cholesterol p < 0,001 HDL-cholesterol p < 0,01 LDL-cholesterol Total cholesterol/HDL cholesterol ratio Fasting triglyceride p < 0,0001
 Smoking - ex. - current. p < 0,01** p < 0,0001** p < 0,05** Blood pressure - systolic. - diastolic. p < 0,05. N.S. Total cholesterol. p < 0,001. HDL-cholesterol. p < 0,01. LDL-cholesterol. Total cholesterol/HDL cholesterol ratio. Fasting triglyceride. p < 0,0001.")
48
Kempler P, Tesfaye S, Chaturvedi N. et al
Kempler P, Tesfaye S, Chaturvedi N. et al. Autonomic neuropathy is associated with increased cardiovascular risk factors: the EURODIAB IDDM Complications Study. Diabetic Med 2002; 19: * adjusted for age, duration and HbA1C Adjusted*relative risk of abnormal R-R ratio (p-value, testing for trend) Peripheral neuropathy p < 0,0001 Albumin excretion Retinopathy Severe hypoglycaemia p = 0,03 Severe ketoacidosis Cardiovascular disease
 Peripheral neuropathy. p < 0,0001. Albumin excretion. Retinopathy. Severe hypoglycaemia. p = 0,03. Severe ketoacidosis. Cardiovascular disease.")
49
Stella et al. Cardiac autonomic neuropathy (expiration and inspiration ratio) in type 1 diabetes. Incidence and predictors. J Diab Compl 2000;14:1-6 Significant independent predictors of CAN: age (RR: 2.15, p=0,0001) HbA1c (RR: 1.50, p=0,0002) nephropathy (albumin excretion>200ug/min) (RR: 2.46, p=0,0001) Hypertension was predictive if nephropathy was not included in the model.
 HbA1c (RR: 1.50, p=0,0002) nephropathy (albumin excretion>200ug/min) (RR: 2.46, p=0,0001) Hypertension was predictive if nephropathy was not included in the model.")
50
Risk factors for incidence of neuropathy
Development of Neuropathy at FU Tesfaye et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:

51
Risk factors for incidence of neuropathy
Development of Neuropathy at FU Tesfaye et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:

52
Risk factors for incidence of neuropathy
Development of Neuropathy at FU Tesfaye et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:

53
Risk factors for for incidence of neuropathy after adjusting for age and HbA1c
Development of Neuropathy at FU

54
Conclusions The incidence of neuropathy over approximately a 7 year period was 25% Independent risk factors for incidence were age, HbA1c, cholesterol, fasting triglyceride, presence of CVD at baseline and presence of retinopathy at baseline Existence of previous CVD independently increased the risk of neuropathy threefold Vascular factors macrovascular disease microvascular complications Tesfaye et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:

55
Eurodiab: 276/1172 patients developed neuropathy in 7.3y
Risk Factors for Neuropathy after Adjustment for HBA1c and Duration of Diabetes Eurodiab: 276/1172 patients developed neuropathy in 7.3y Variable Odds Ratio P value CVD 2.74 <0.0001 Albuminuria 1.48 0.02 Hypertension 1.92 <0.001 Smoking 1.55 BMI 1.40 Triglycerides 1.35 Total Cholesterol 1.26 0.001 LDL-C 1.22 Tesfaye et al NEJM 352: ,2005

56
A diabeteses neuropathia oki kezelése
Optimális anyagcserehelyzet biztosítása Rizikófaktorok befolyásolása Benfotiamin Alpha-liponsav

57
A multifaktoriális intervenció hatékonysága – Steno-2
Mikrovaszkuláris szövődmények Makrovaszkuláris szövődmények RR 0,47 (95% CI 0,22-0,74, P=0,01) n = 160, DM2T, Gaede P et al. N Engl J Med 348: , 2003
 n = 160, DM2T, Gaede P et al. N Engl J Med 348: ,")
58
”Take home message” A hagyományos cardiovascularis rizikófaktorok szerepe nemcsak a macrovascularis, hanem a microvascularis szövődmények kialakulása szempontjából is meghatározó fontosságú.

59
A tudomány csalhatatlan, de a tudósok mindig tévednek
Anatole France

60
The epidemiologist can confuse the non-epidemiologist
Japanese eat very little fat and suffer far less from heart attack than British or American French eat a lot of fat and suffer far less from heart attack than British or American Japanese drink very little red vine and suffer far less from heart attack than British or American French and Italian drink lot of red vine and suffer far less from heart attack than British or American A. Adler, EDEG, Oxford, 2002.

61
The epidemiologist can confuse the non-epidemiologist
Conclusion: You can eat as you want English speaking will kill you A. Adler, EDEG, Oxford, 2002.

Hasonló előadás












 MORE?” symposium Washington.>")







