Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Haemolyticus uraemiás szindróma
Dr. Túri Sándor SZTE Gyermekgyógyászati Klinika, Szeged 1

2
A HAEMOLYTICUS URAEMIÁS SZINDRÓMA TÜNETEI
HAEMOLYTICUS ANAEMIA THROMBOCYTOPENIA NEPHROPATHIA MICROANGIOPATHIA NEUROPATHIA 2

3
Haemolyticus uraemiás szindróma és a thrombocytus thrombocytopeniás purpura etiológiai felosztása (1) Haemolyticus uraemiás szindróma Fertõzés utáni E. coli 0157 H:7 Shigella dysenteriae neuraminidáztermelõ kórokozókhoz társult egyéb infekciók Sporadikus, nem fertõzéshez társult öröklött autoszomális recesszív autoszomális domináns gyógyszer okozta cyclosporin A, mitomycin C oralis anticoncipiensek terhességhez társult szisztémás lupus erythematodeshez kapcsolódó transzplantációhoz társult sclerodemával jelentkezõ carcinomához társult 3

4
Thromboticus thrombocytopeniás purpura Idiopathiás Szekunder
Haemolyticus uraemiás szindróma és a thrombocytus thrombocytopeniás purpura etiológiai felosztása (2) Thromboticus thrombocytopeniás purpura Idiopathiás Szekunder szisztémás lupus erythematodeshez társult carcinomához társult HIV-1-hez társult öröklött gyógyszer okozta kokain, quinidin A haemolyticus uraemiás szindróma szövettani felosztása fõleg glomeruláris érintettség (kisgyermekekben) főleg vascularis érintettség (nagyobb gyermekekben) akut corticalis nekrózis 4
 Thromboticus thrombocytopeniás purpura. Idiopathiás. Szekunder. szisztémás lupus erythematodeshez társult. carcinomához társult. HIV-1-hez társult. öröklött. gyógyszer okozta. kokain, quinidin. A haemolyticus uraemiás szindróma szövettani felosztása. fõleg glomeruláris érintettség (kisgyermekekben) főleg vascularis érintettség. (nagyobb gyermekekben) akut corticalis nekrózis. 4.")
6
CONTROL ACUTE HUS in HUS FAMILY
HUS REMISSION MEMBERS

13
KLINIKAI TÜNETEK D + HUS: homogén entitás
vero/shiga toxin kóroki szerepe prodromális betegség: akut gastroenteritis rapid kezdet: szinkronban hemolízis, thrombocytopénia, azotémia gyermekeken gyakoribb, mint felnõttekben ritkán recidivál jó prognózis 7

14
Bevezetõ gastrointestinális tünetek
Elkülönítendõ: colitis ulcerosa appendicitis invaginatio rectalis prolapsus gastroenteritis akut bakteriális enterocolitis Chron betegség (1–15 nap) hasi fájdalom hányás véres hasmenés 8
 hasi fájdalom. hányás. véres hasmenés. 8.")
15
Véralvadási rendszer HUS-ban
THROMBOCYTA IN VITRO AGONIS- TÁKRA ¯ ALVADÁSI FAKTOROK PI NORM. PTI NORM. FIBRINOGEN NORM. V. FAKTOR NORM. VIII. FAKTOR FDP VIII. FAKTOR MULTIMER FIBRONECTIN ¯ SZÁM ÉLETTARTAM AGGREGÁCIÓ 4 FAKTOR SZÉRUM THROMBOCYTA BETA-THROMBOGLOBULIN SZÉRUM THROMBOCYTA SEROTONIN SZÉRUM 14

16
Vesefunkció rapid beszûkülése
szérum kreatinin, UN, K, foszfor, húgysav fokozott metabolikus acidózis szérum Na, Ca, HCO3, albumin csökkent szérum koleszterin, triglicerid, foszfolipid fokozott Oliguria miatt congestiv szívelégtelenség (lehet iatrogén is) kisvérköri pangás hypertonia Agyoedema, központi idegrendszeri tünetek (irritabilitás, aluszékonyság, görcsök, kóma) hypertonia, microthrombusok, agyvérzés súlyosbítják hemiparesis, kérgi vakság, agytörzsi érintettség 10
 kisvérköri pangás. hypertonia. Agyoedema, központi idegrendszeri tünetek. (irritabilitás, aluszékonyság, görcsök, kóma) hypertonia, microthrombusok, agyvérzés súlyosbítják. hemiparesis, kérgi vakság, agytörzsi érintettség. 10.")
17
Elektrolit és metabolikus rendellenességek HUS-ban
metabolikus acidózis Se Na /¯ K húgysav összfehérje/albumin ¯ lipidek máj enzimek (SGOT, SGPT, LDH, GGTP) Bi Ca ¯ P 11
 Bi Ca ¯ P 11.")
18
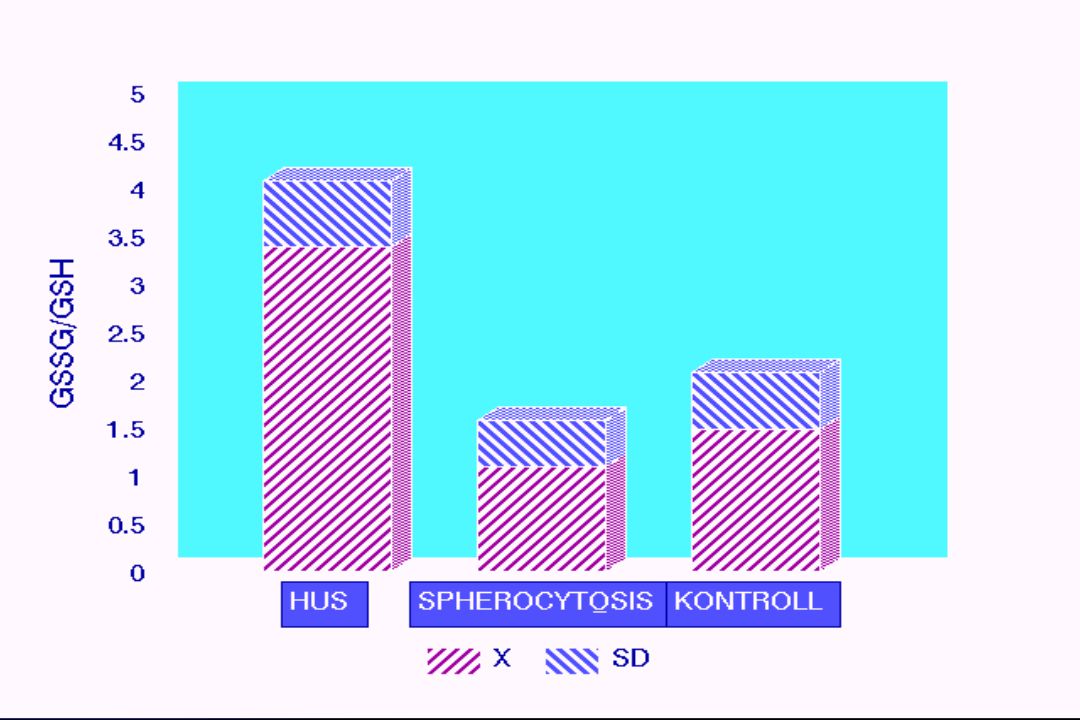
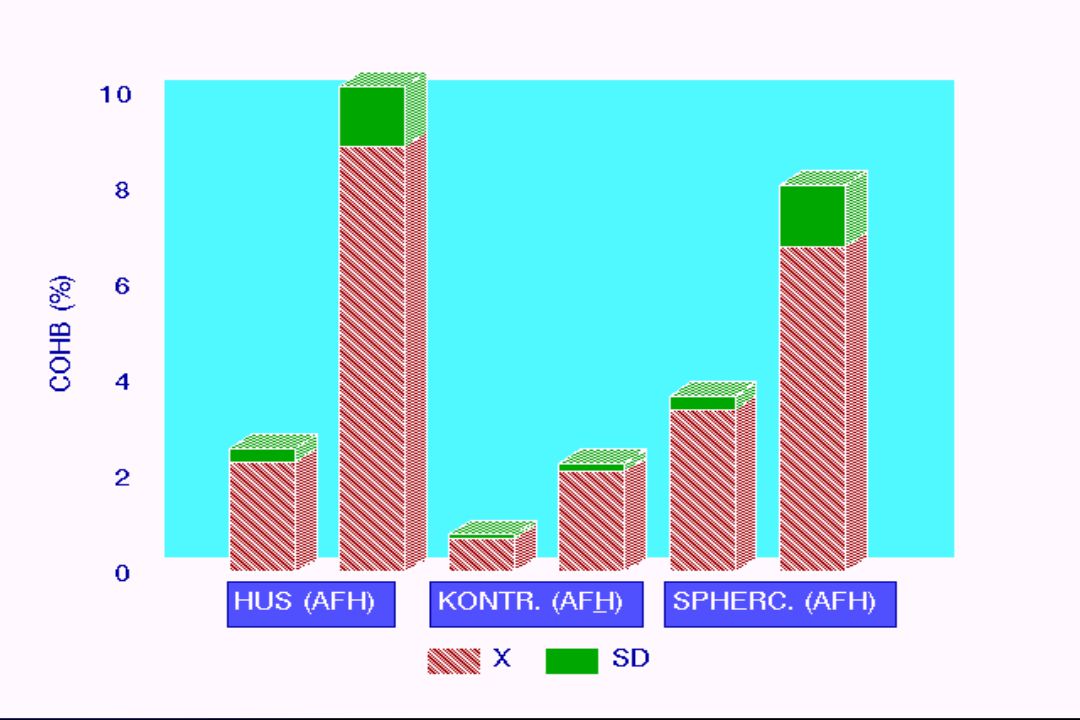
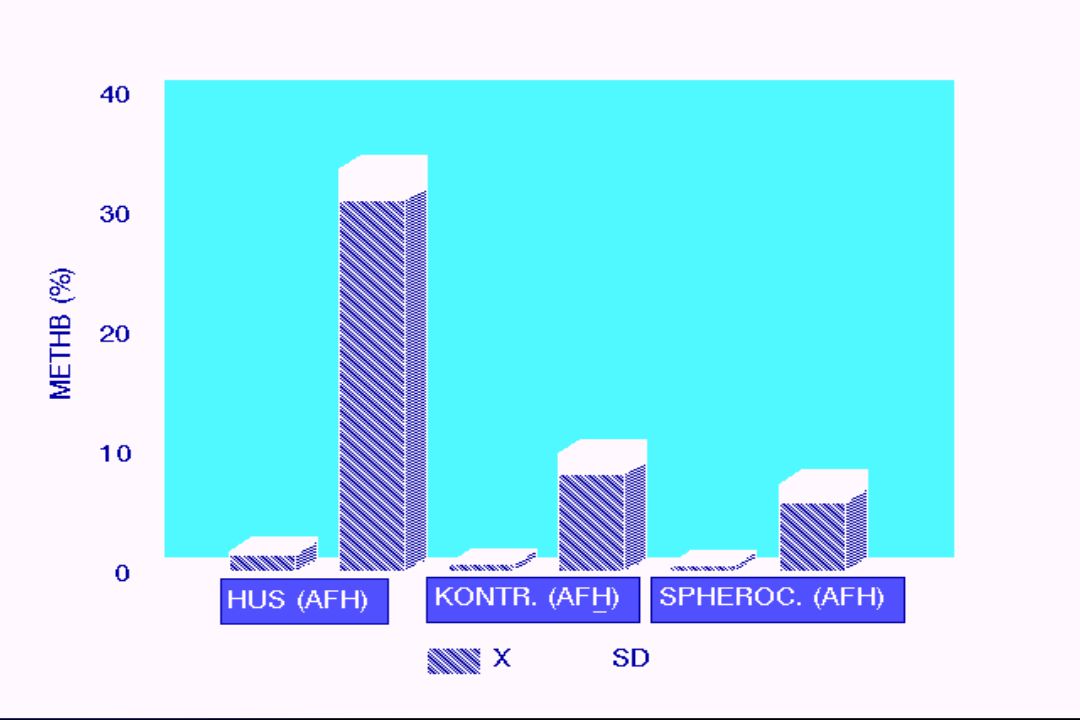
Hematológiai tünetek hemolitikus anémia (fragmentocytosis, COHb-,
MetHb-, LDH-, szérum bilirubin fokozott, reticulocytosis +/-, Coombs teszt negatív, haptoglobin szint alacsony) petechiák, buccalis nyálkahártyavérzések 12
 petechiák, buccalis nyálkahártyavérzések. 12.")
19
Atípusos (D-) haemolyticus uraemiás szindróma
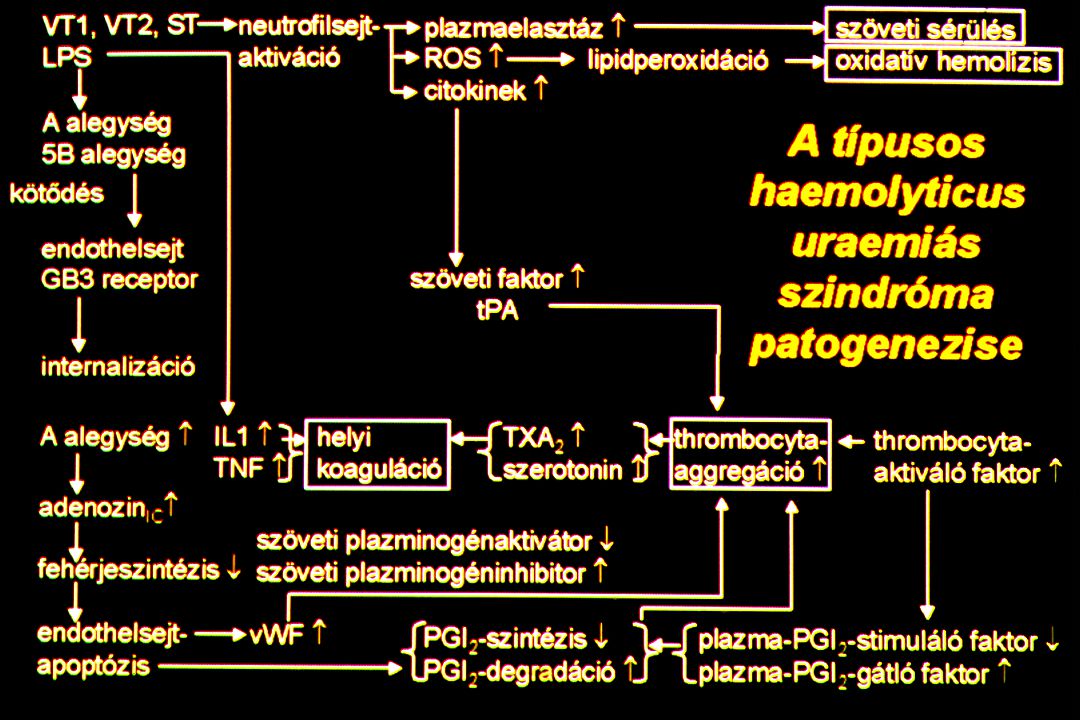
hiányzik a véres hasmenés tünetek aszinkron manifesztálódása prognózis sokkal rosszabb (mortalitás: 70%) Pathogenesis: prosztaciklin defektus citokin felszabadulás neutrophil aktiváció reaktív oxigén gyökök thrombocyta aktiváció von Willebrandt f. felszaporodás Etiológia: heterogén 17
 Pathogenesis: prosztaciklin defektus. citokin felszabadulás. neutrophil aktiváció. reaktív oxigén gyökök. thrombocyta aktiváció. von Willebrandt f. felszaporodás. Etiológia: heterogén. 17.")
20
90% of pediatric cases due to Shiga toxin- E. coli (O157:H7)
10% are atypical cases with other causes of these, 40% pneumococcus origine 50% disorders of complement thrombotic thrombocytopenic purpura (TTP) TTP-HUS spectrum of related disorders TTP has same manifestations, PLUS … neurologic involvement fever ETIOLOGY OF HEMOLYTIC-UREMIC SYNDROME Cochran, JB, 2004, Pediatr Nephrol 19:
 TTP-HUS spectrum of related disorders. TTP has same manifestations, PLUS … neurologic involvement. fever. ETIOLOGY OF HEMOLYTIC-UREMIC SYNDROME. Cochran, JB, 2004, Pediatr Nephrol 19:")
21
HEMOLYTIC-UREMIC SYNDROME
CLINICAL SPECTRUM OF TTP-HUS Veyradier, A, 2001, Blood 98:

22
ATYPICAL HUS Other causes of atypical hemolytic-uremic syndrome
Other pathogens S. pneumoniae HIV Q fever CMV Staphylococcus Hantavirus Drugs cyclosporine bleomycin tacrolimus cisplatin mitomycin Underlying medical conditions Upshaw-Shulman syndrome MCP deficiency factor H deficiency factor I deficiency cobalamin-C disease Cochran, JB, 2004, Pediatr Nephrol 19:

23
Légúti infekcióhoz társult HUS
Neuraminidázt termelõ baktériumok (pneumococcus, stb.), ricketsiák, vírusok hatására endothel sejtek leukocyták thrombocyták elvesztik szialoprotein tartalmukat a sejtmembránból. Felszínre kerül a Thomsen–Friedenreicht (T) antigén a plazmában jelen van a T-antitest (IgM-típusú) Vvt-k, thrombocyták hemagglutinációját okozza (álpozitív Coombs teszt) 19
, ricketsiák, vírusok hatására. endothel sejtek. leukocyták. thrombocyták elvesztik szialoprotein tartalmukat a sejtmembránból. Felszínre kerül a Thomsen–Friedenreicht (T) antigén. a plazmában jelen van a T-antitest (IgM-típusú) Vvt-k, thrombocyták hemagglutinációját okozza. (álpozitív Coombs teszt) 19.")
24
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
DRUG-ASSOCIATED cyclosporine/tacrolimus-associated mechanism unclear seen in solid-organ or stem-cell transplantation, and non-transplant estimated incidence of 1-5% following stem-cell transplantation no clear dose-response association to risk usually observed in first 6 months after transplantation disease can be localized or systemic events associated with higher rate of graft loss or mortality therapeutic interventions treat co-inciting factors (CMV infection) dose reduction withhold drug, switch to alternate drug plasma exchange transfusion corticosteroids IVIG also reported with Campath (alemtuzumab, anti-CD52) Zakarija A, et al, 2005, Semin Thromb Hemost 31:
 dose reduction. withhold drug, switch to alternate drug. plasma exchange transfusion. corticosteroids. IVIG. also reported with Campath (alemtuzumab, anti-CD52) Zakarija A, et al, 2005, Semin Thromb Hemost 31:")
25
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
UPSHAW-SHULMAN SYNDROME congenital deficiency of ADAMTS-13 protease cleaves vWF multimers presents at birth with hemolytic anemia and thrombocytopenia renal involvement develops later in life inhibitor auto-antibodies to ADAMTS-13 can also cause similar syndrome Brass, L, 2001, Nature Med 7:

26
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
COBALAMIN-C DEFICIENCY disorder of vitamin B12 (cobalamin) metabolism hyperhomocysteiemia methylmalonic aciduria presents with atypical HUS and neurological symptoms early onset seizures hypotonia developmental delay retinopathy macrocytic anemia neutropenia Role of cobalamin in homocysteine and methylmalonic acid metabolism. Panel A - Methylcobalamin is a cofactor in the synthesis of methionine from homocysteine. Panel B - Adenosylcobalamin is a cofactor in the synthesis of succinyl-CoA from methylmalonyl-CoA. Tetrahydrofolate (THF) participates in homocysteine but not methylmalonic acid (MMA) metabolism. Thus, cobalamin deficiency is characterized by elevations in the serum levels of both homocysteine and MMA, while only homocysteine levels are elevated in folate deficiency. Tefferi, A, et al, 1994, Mayo Clin Proc 69:
 metabolism. hyperhomocysteiemia. methylmalonic aciduria. presents with atypical HUS and neurological symptoms. early onset seizures. hypotonia. developmental delay. retinopathy. macrocytic anemia. neutropenia. Role of cobalamin in homocysteine and methylmalonic acid metabolism. Panel A - Methylcobalamin is a cofactor in the synthesis of methionine from homocysteine. Panel B - Adenosylcobalamin is a cofactor in the synthesis of succinyl-CoA from methylmalonyl-CoA. Tetrahydrofolate (THF) participates in homocysteine but not methylmalonic acid (MMA) metabolism. Thus, cobalamin deficiency is characterized by elevations in the serum levels of both homocysteine and MMA, while only homocysteine levels are elevated in folate deficiency. Tefferi, A, et al, 1994, Mayo Clin Proc 69:")
27
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
FACTOR H DEFICIENCY thought to account for 10-22% of atypical HUS cases reported in both familial and sporadic forms usually presents in infancy or early childhood, but may present in adulthood one study of 16 FH-deficient patients 6 with homozygous deficiency 4 had membranoproliferative glomerulonephritis 2 had atypical HUS 10 had heterozygous deficiency all developed atypical HUS homozygotes had low levels of FH, C3, FB and CH50 heterozygotes had low to normal values Dragon-Durey, M-A, et al, 2004, J Am Soc Nephrol 15:

28
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
FACTOR I DEFICIENCY reported only in sporadic forms of atypical HUS in one study, 2 out of 76 patients with atypical HUS had FI deficiency most reported cases involve heterozygous mutations no increased susceptibility to infection homozygous FI deficiency associated with increased infection susceptibility encapsulated organisms (meningococcus, pneumococcus, hemophilus) acquired C3 deficiency due to uncontrolled consumption Dragon-Durey, M-A, et al, 2005, Springer Semin Immun 27: Kavanagh, D, et al, 2005, J Am Soc Nephrol 16:
 acquired C3 deficiency due to uncontrolled consumption. Dragon-Durey, M-A, et al, 2005, Springer Semin Immun 27: Kavanagh, D, et al, 2005, J Am Soc Nephrol 16:")
29
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
COMPLEMENT DYSREGULATION outcomes of atypical HUS overall 50% of patients develop ESRD 25% mortality during acute illness end-stage renal disease 70% with FH-deficiency HUS develop ESRD or die >60% with FI-deficiency HUS develop ESRD 86% with MCP-deficiency HUS remain dialysis-free 70% had recurrence of HUS Richards, A, 2007, Mol Immunol 44:

30
Recidiv haemolyticus uraemiás szindróma
vesetranszplantáció után orális fogamzásgátlók mellett terhességhez társultan idiopathiásan 20

31
Familiaris haemolyticus uraemiás szindróma
Klinikai tünetek: nincs diarrhoeás prodróma progresszív lefolyás rekurrálhat a transzplantátumban is Szövettan: arterioláris elváltozások orális fogamzásgátlók, terhesség kerülendõ Formái: 1. Napokon-heteken belül még egy családtag megbetegszik. prognózis jó. 2. Két családtag betegsége között több, mint egy év telik el. mortalitás 65%. 3. Autoszom domináns öröklõdés. alacsony C3 komplement, PGI2 defektus. 21

32
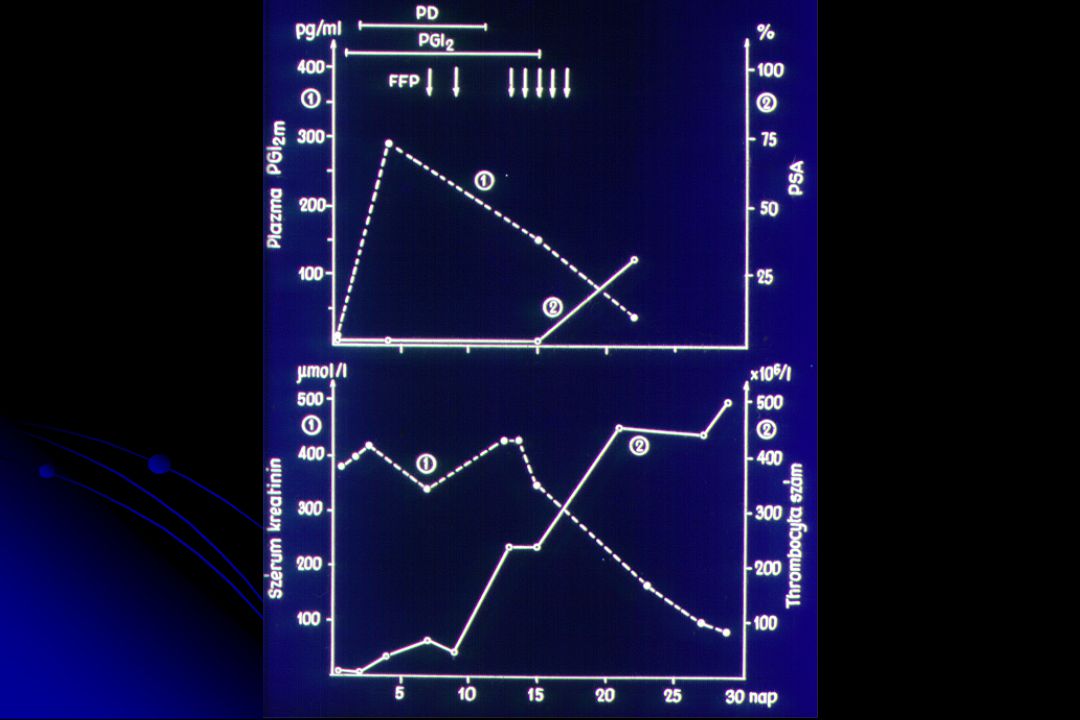
PGI2 INFÚZIÓ, THROMBOCYTA AGGR. GÁTLÓK
A HUS KEZELÉSE DIALYSIS (pd, hd) VVT TRANSZFÚZIÓ PLAZMAFEREZIS ANTIOXIDÁNS TH. PGI2 INFÚZIÓ, THROMBOCYTA AGGR. GÁTLÓK 22
 VVT TRANSZFÚZIÓ. PLAZMAFEREZIS. ANTIOXIDÁNS TH. PGI2 INFÚZIÓ, THROMBOCYTA AGGR. GÁTLÓK. 22.")
33
Access Devices and Plt < 50k
Address Thrombocytopenia Transfuse for: Symptomatic Bleeding Pre-op for Vascular Access Devices and Plt < 50k Most would agree to be overly cautious/conservative with plt transfusions, as they provide more substrate for the pathologic process. Most would agree to be overly cautious/conservative with plt transfusions, as they provide more substrate for the pathologic process.

34
Experimental Therapies Primary Treatment Eculizimab Cryopoor FFP
Plasmapheresis/ Exchange Anti-platelet Agents Anti-coagulants / fibrinolytics Vitamin E IVIG PGI2 Infusion Lasix with Replacement IVF Experimental Therapies Pts tx’ed with FFP had less cortical necrosis than those without FFP beneficial in non-diarheal HUS FFP contraindicated in pneumococcal HUS The management I’ve just discussed will be adequate for the majority of cases. However, some cases, especially the non-diarrheal HUS such as pregnancy, mitomycin, & rheumatologic disease, will be refractory. There are many experiemtnal therapies, most of them unproven, which will become the second line in such cases. Cryopoor FFP is - coagulation proteins. Pts tx’ed with FFP had less cortical necrosis than those without FFP beneficial in non-diarheal HUS FFP contraindicated in pneumococcal HUS IVIG Ped Neph 5:289: Lasix HUS ARF ? 2/2 uriacid nephropathy. try Lasix 2-3/mg/kg q4hr with UO repl Lasix not prevents saturation but is non-uricosuric (Clin Neph 30:207) HUS ARF is a uriacid nephropathy. Try Lasix 2-3/mg/kg q4hr it is non-uricosuric
 HUS ARF is a uriacid nephropathy. Try Lasix 2-3/mg/kg q4hr it is non-uricosuric.")
37
Újabb terápiás lehetõségek (1)
A fokozott oxidatív stressz, csökkent antioxidáns védelmi mechanizmusok alapján E-vitamin kezelés, taurin-trikarboxilsav, von Willebrand-faktorhoz kötõdve megakadályozza a thrombocyták glikoprotein Ib-, IIb- és IIIa-receptoraihoz kapcsolódását. 25

38
Újabb terápiás lehetõségek (2)
Rekombináns von Willebrand-faktor, leszorítva ezzel a nagy von Willebrand-faktor-multimereket a thrombo-cytaglikoprotein Ib-receptorokról. Atípusos, öröklõdõ haemolyticus uraemiás szindróma esetén a graftban való recidíva veszélye miatt az élõ donortól történõ vesetranszplantáció nem ajánlott. 26

39
4

40
KLINIKAI TÜNETEK TTP: bizonytalan kezdet aszinkron manifesztáció
neurológiai tünetek dominálnak véres széklet ritka gyermekeken ritka prognózisa bizonytalan plazmaferezis hatásos lehet 28

41
Terápia thromboticus thrombocytopeniás purpurában a plazmaferezis elõnyös hatású terhességben manifesztálódott thrombocitus thrombocytopeniáspurpura esetén, ha az antitrombin III-szint normális, plazmaferezist, ill. a 34. gestatiós hét után a szülés beindítását javasolják antikoaguláns-fibrinolízist gátló, szteroidterápia sem HUS-ban, sem TTP-ben nem ajánlott kivéve ha komplement defektus van. prosztaciklininfúzió indikációjáról megoszlanak a vélemények. 3–5 ng/kg/óra adagban alkalmazzák 29

43
Thromboticus thrombocytopeniás purpura
Láz haemolyticus anaemia, thrombocytopeniás purpura, fluktuáló neurológiai zavarok aszinkron manifesztációval kezdetben neurológiai tünetek az agyi érintettség a thromboticus occlusio következménye uremia viszonylag ritka, gyakori haematuria, proteinuria leukocytosis, balra tolt vérkép gyermekek esetében – a felnőttekhez képest – elvétve fordul elõ 27

44
Thromboticus thrombocytopeniás purpura
Neutrophilaktiváció, proteolitikus enzim- és szabadgyök-felszabadulás, prosztaciklin hiány, thrombocytaaktiváció, lokális thrombosis és fibrindepozíció von Willebrand-faktor-termelés és -felhasználás a thromboticus microangiopathia (TMA) olyan veselaesio, melyben glomerulusokban és arteriolákban thrombusok vannak
 olyan veselaesio, melyben glomerulusokban és arteriolákban thrombusok vannak.")
45
Patológia 1. Kisgyermekekben
a kapillárisfal megvastagodik, az endothelsejtek duzzadtak szûkületet vagy elzáródást okoznak az arteriolaris érintettség rendszerint minimális 2. Nagyobb gyermekek és felnõttek arteriolaris elváltozások a glomerularis elváltozások mellett szerepe van a hypertonia kialakulásában az interlobaris arteriákban thrombusok láthatók intimaoedemával és myointimalis sejtproliferációval különbözõ stádiumban szervülõ arteriolaris és kapilláris microthrombusok mutathatók ki 5

47
Thomsen-Friedenreich Ag, HUS, & Hemolysis
Pneumococcal Neuraminidase TF TF

48
ARF Low Blood Pressure Hypoxia Nephrotoxins Endothelin Angiotensin
Reperfusion: O2 radicals Medullary hypoxia Decreased RBF ATP depletion Capillary leak Cell swelling Destruction F-aktin/integrins Loss of cell polarity Decreased Kf „Medullary congestion” Cell desqumation Decreaased Na+ transport Tubular obstruction Aggregation of THP „Backleak” Low GFR Activation of TGF

50
A haemolyticus uraemiás szindróma patomechanizmusa
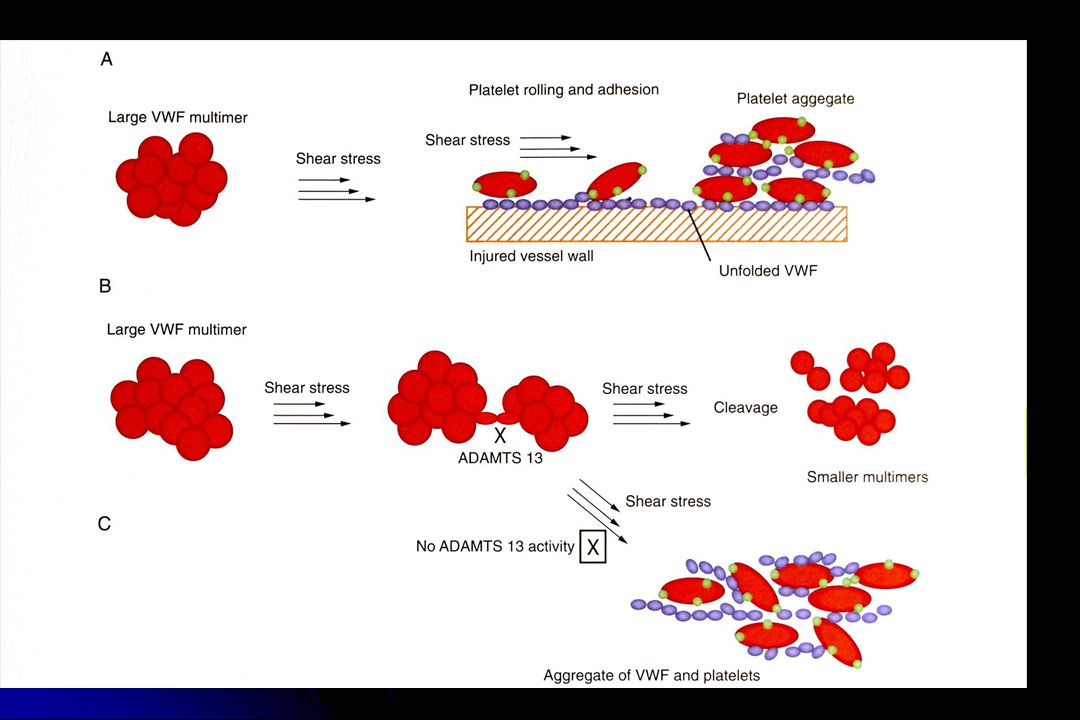
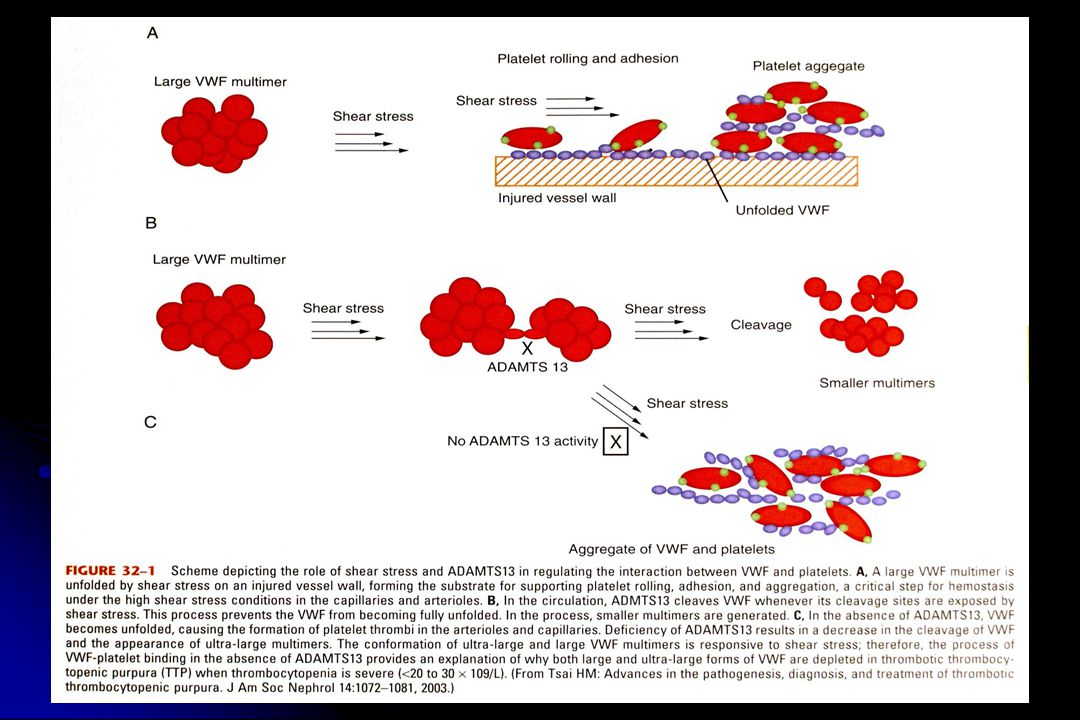
Verotoxin (E. Coli 0157), shiga toxin neutrophil aktiváció cytokin és szabad oxigén gyök release thrombocyta aktiváció, érfal károsodás, oxidatív haemolysis diffúz intravascularis coagulacio Willebrand-faktor multimer PGI2 defektus (termelés, hatás stimuláló és gátló faktorok) fibrinolysis elégtelensége (plazminogen aktivátor gátlása) vagy: neuraminidase termelö kórokozók sialsav bontása, a vérsejtek és az endothel károsodása reaktív oxigén gyök release Thomsen Friedenreich antigén felszínre kerül haemaglutináció 6
, shiga toxin. neutrophil aktiváció. cytokin és szabad oxigén gyök release. thrombocyta aktiváció, érfal károsodás, oxidatív haemolysis. diffúz intravascularis coagulacio. Willebrand-faktor multimer. PGI2 defektus (termelés, hatás stimuláló és gátló faktorok) fibrinolysis elégtelensége (plazminogen aktivátor gátlása) vagy: neuraminidase termelö kórokozók. sialsav bontása, a vérsejtek és az endothel károsodása. reaktív oxigén gyök release. Thomsen Friedenreich antigén felszínre kerül. haemaglutináció. 6.")
52
Cyclosporine/Tacrolimus
ATYPICAL HEMOLYTIC-UREMIC SYNDROME DRUG-ASSOCIATED Cyclosporine/Tacrolimus Sirolimus Stepkowski, SM, 2000, Exp Rev Mol Med fig002ssh, fig003ssh.

53
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
PNEUMOCOCCAL-ASSOCIATED pathogenesis microbial neuraminidase exposes Thomsen-Friedenreich (T) antigen cryptic T-antigen found on erythrocytes, platelets, and glomeruli overexpressed by carcinoma neuraminidase cleaves sialic acid, exposing T-antigen bound by “natural” anti-T IgM antibodies results in thrombotic microangiopathy Cochran, JB, 2004, Pediatr Nephrol 19:
 antigen. cryptic T-antigen found on erythrocytes, platelets, and glomeruli. overexpressed by carcinoma. neuraminidase cleaves sialic acid, exposing T-antigen. bound by natural anti-T IgM antibodies. results in thrombotic microangiopathy. Cochran, JB, 2004, Pediatr Nephrol 19:")
54
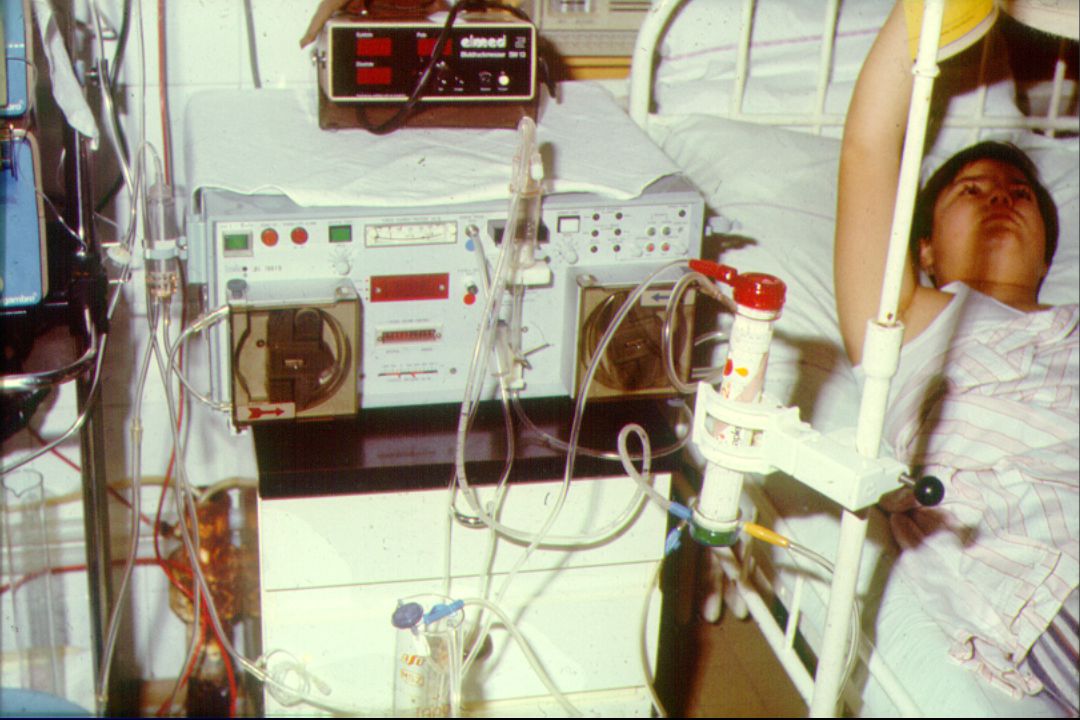
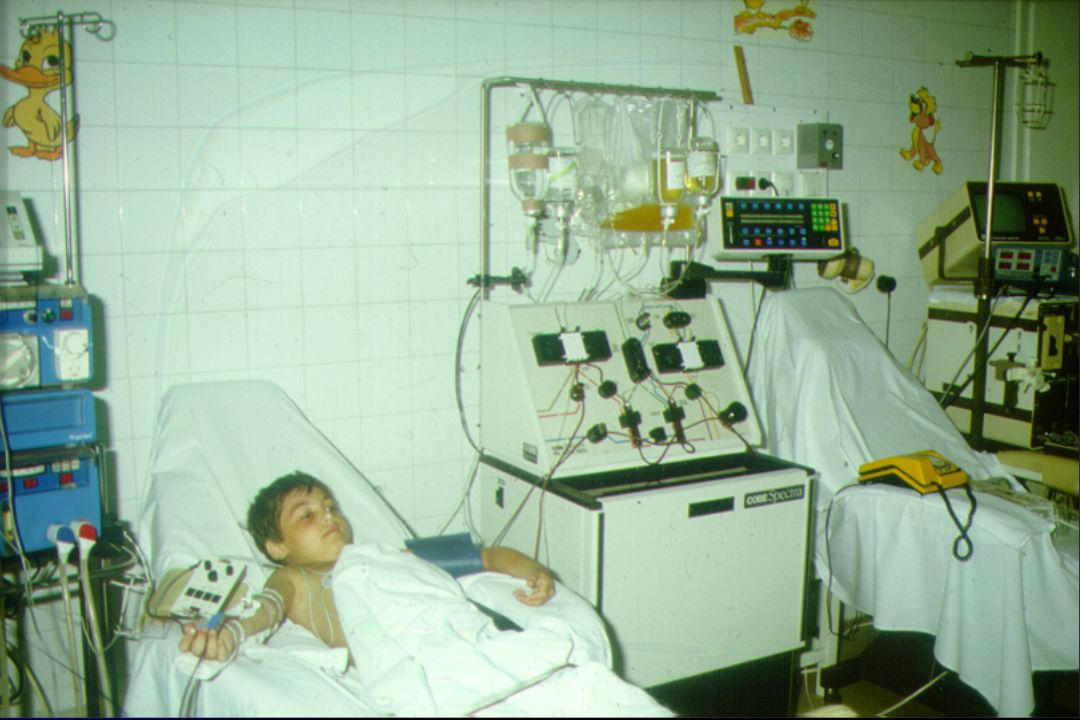
DIALIZIS KEZELÉS AKUT VESEELÉGTELENSÉGBEN
Peritonealis dializis CAPD szerelék (zárt rendszer) Tenkchoff katéter Seldinger módszer (subcutan alagút) Partialis omentectomia 1,25 %, 2.5 % Glukoz- 135 mM NaCl oldat Töltési volumen: ml/kg Töltési idő: perc Hemodializis (6 év felett), bicarbonat HD, HDF i.v. kanül 80 ml/p vérátáramlás 1.5-2 óra/nap
 Tenkchoff katéter. Seldinger módszer (subcutan alagút) Partialis omentectomia. 1,25 %, 2.5 % Glukoz- 135 mM NaCl oldat. Töltési volumen: ml/kg. Töltési idő: perc. Hemodializis (6 év felett), bicarbonat HD, HDF. i.v. kanül. 80 ml/p vérátáramlás óra/nap.")
55
ATYPICAL HEMOLYTIC-UREMIC SYNDROME COMPLEMENT DYSREGULATION
pathogenesis of atypical HUS activates complement cascade and C3a/C5a C3a/C5a attract leukocytes, producing TNF and IL-8 cytokines cause endothelial damage and exposure of extracellular matrix infection/inflammation increases rate of C3b formation ECM exposure amplifies deposition of C3b and complement activation lack of normal factor H, factor I, or MCP results in unchecked activation progressive tissue damage occurs

56
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
COMPLEMENT DYSREGULATION treatment plasma exchange and plasma infusions of FFP 32 FH-deficient patients treated with FFP 67% in remission similar results in FI-deficient patients MCP-deficiency not amenable to FFP infusions or plasma exchange renal transplantation protective renal transplantation 30 FH-deficient patients underwent renal transplantation 80% had disease recurrence 6 FI-deficient patients underwent renal transplantation 100% had disease recurrence transplanted MCP-deficient patients 10 MCP-deficient patients transplanted 1 had recurrence of HUS low C3 and factor B levels – disease modifiers? Richards, A, 2007, Mol Immunol 44:

57
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
COMPLEMENT DYSREGULATION complement components and pathways Janeway, C, et al, Immunobiology, New York: Garland Science, 2005.

58
ATYPICAL HEMOLYTIC-UREMIC SYNDROME
COMPLEMENT DYSREGULATION FH, FI, and MCP deficiency have incomplete penetrance disease modifiers or other factors may have role environmental triggers infections preceded 70% of those with FH mutation 60% of those with FI mutation 100% of cases of HUS in MCP-mutants pregnancy trigger in 4% of FH-HUS 40% of FI-HUS multiple-hits one pedigree in which atypical HUS occurred only with inheritance of ALL: MCP P131S mutation MCP promoter polymorphism dinucleotide insertion into FI gene resulted in 50% expression level of each protein Richards, A, 2007, Mol Immunol 44:

59
A COMPLEMENT RENDSZER RENDELLENESSÉGEINEK SZŰRÉSE aHUS-ban
Se C3, Faktor B, H, és I Granulocyta MCP szint FH antitestek Genetikai analizis: FH, FI, MCP, FB és C3 Hibrid FH/FHR1 gén MLPA A C3 és a faktor B mutációja a két fő komponens az alternativ komplement aktivációban a C3-konvertáz defetusához, amely predisponál az aHUS kialakulására.

Hasonló előadás