Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Allogén haematopoieticus őssejt transzplantáció Alizadeh Hussain 2015.10.07. Pécs

2
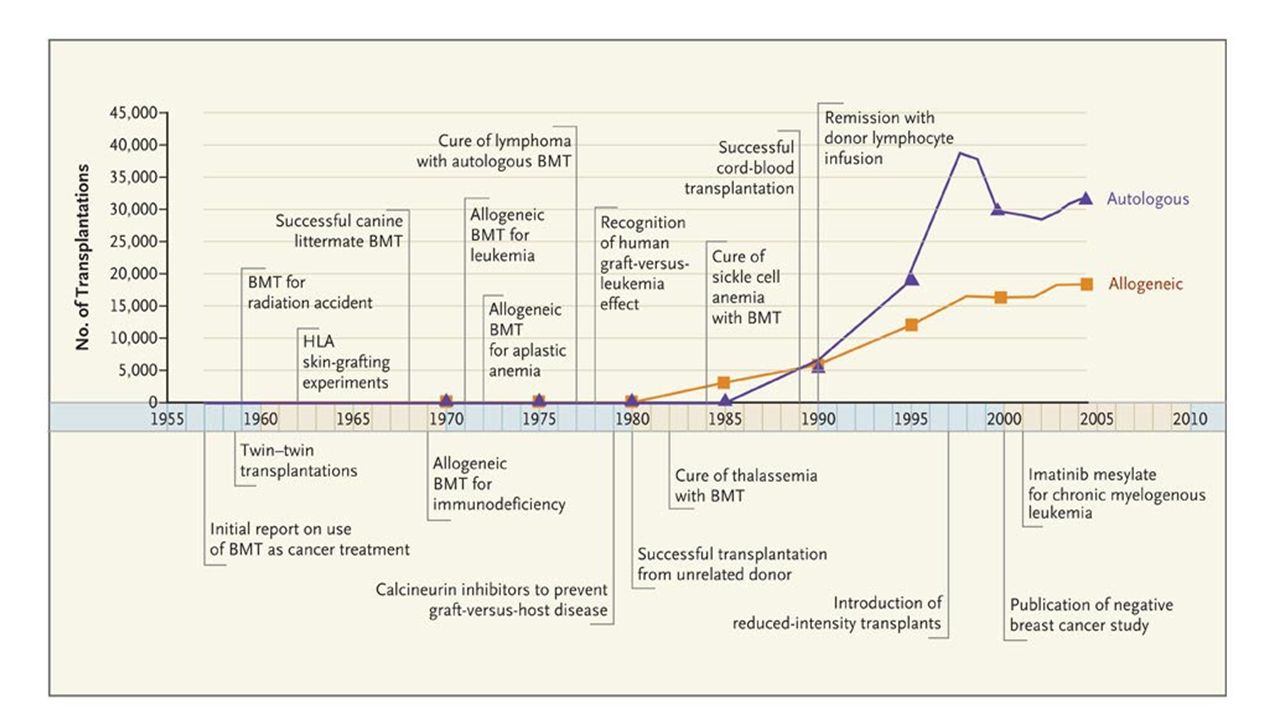
HSCT: Definition Haematopoietic stem cell transplantation (HSCT) is the transplantation of multipotent haematopoietic stem cells, usually derived from bone marrow, peripheral blood, or umbilical cord blood with intention of repopulating/replacing the haematopoietic system in total or in part History: Haematopoietic stem cell transplantation in the mouse the radiation protection phenomenon (mid-1950s) Haematopoietic stem cell tranplantation in the dog Haematopoietic stem cell tranlsplantation in human patients 1959: Georges Mathé performed 1 st European BMT in 5 Yugoslavian nuclear workers 1950s to 1970s: Fred Hutchinson Cancer Research Center Team led by E. Donnall Thomas 1959–1963 : 1 st allogeneic HSCT in humans Beginning of the Modern Era of HSCT: the end of 1960 1968: 1 st physician performed successful BMT was Robert A. Good from University of Minnesota 1975: John Kersey performed 1 st successful BMT to cure a 16-year-old lymphoma patient

3
HSCT: History 1939: Osgood unsuccessfully infused a few milliliters of marrow into patients with AA 1949: Jacobson discovered that shielding the spleen protected mice from lethal irradiation Lorenz performed allogenic BMT in animals protected by total irradiation Lorenz’s findings, and research by Barnes & colleagues, demonstrated that a cellular rather than a humoral factor played a role in graft survival Vanbekkum, DeVries, and other scientists performed important experiments to study immunological reactions in transplantation recipients Initial attempts at allogeneic BMT in the 1950s & 1960s were unsuccessful Later on, HLA system was recognized Getty performed a successful allogeneic marrow graft in a patient with SCID using a sibling donor with identical HLA Two similar successes were reported around the same time These patients did not require IST & survived for > 25 years In the 1970s & 1980s, clinical BMT required matched HLA haplotypes between the donor & recipient

5
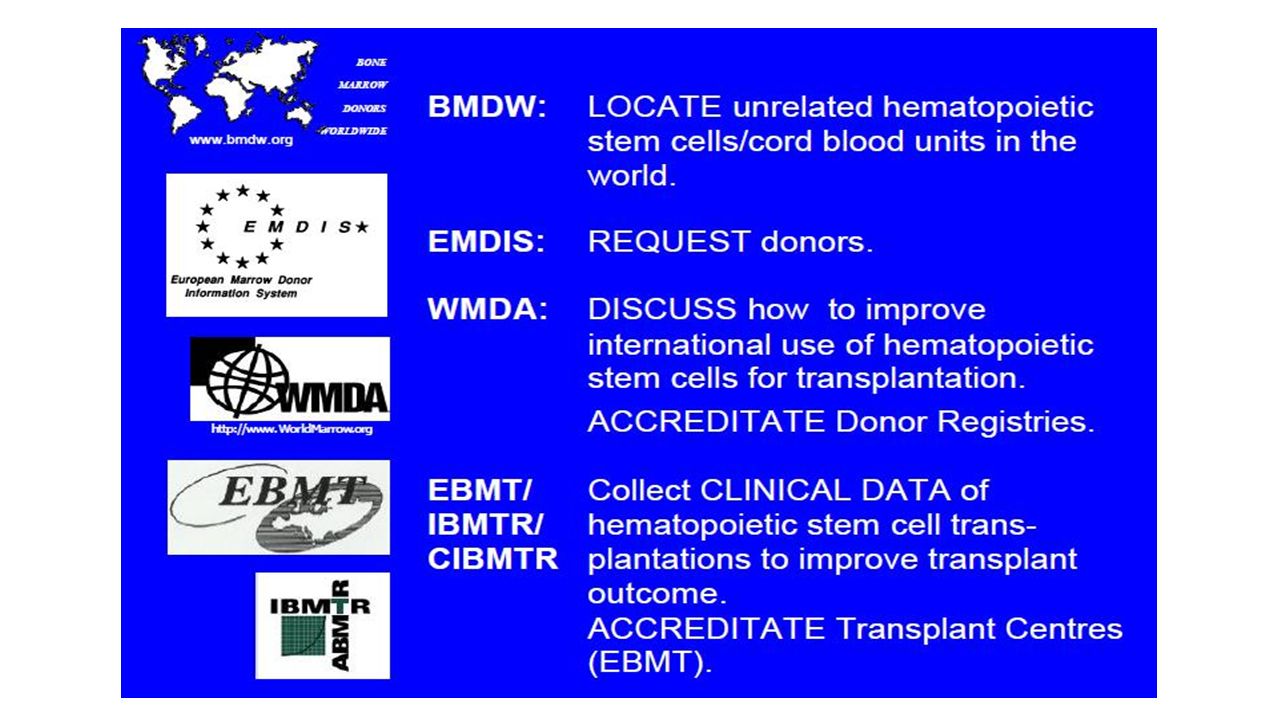
2009 2010 Activations 44201 46919 BMT Tx 3445 (8%) 3574 (8%) PB Tx 8162 (18%) 9248 (20%) CB 3792 (9%) 4036 (9%) TOTtranspl 15399 (35%) 16858 (37%) WMDA 2012
 3574 (8%) PB Tx 8162 (18%) 9248 (20%) CB 3792 (9%) 4036 (9%) TOTtranspl (35%) (37%) WMDA 2012")
7
The Nobel Prize, 1990 E. Donnall Thomas 1 st succsessful HSCT in treatment of acute leukaemias Thomas ED, Lochte HL, Lu WC, Ferrebee JW. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957; 257: 491.

9
Source

10
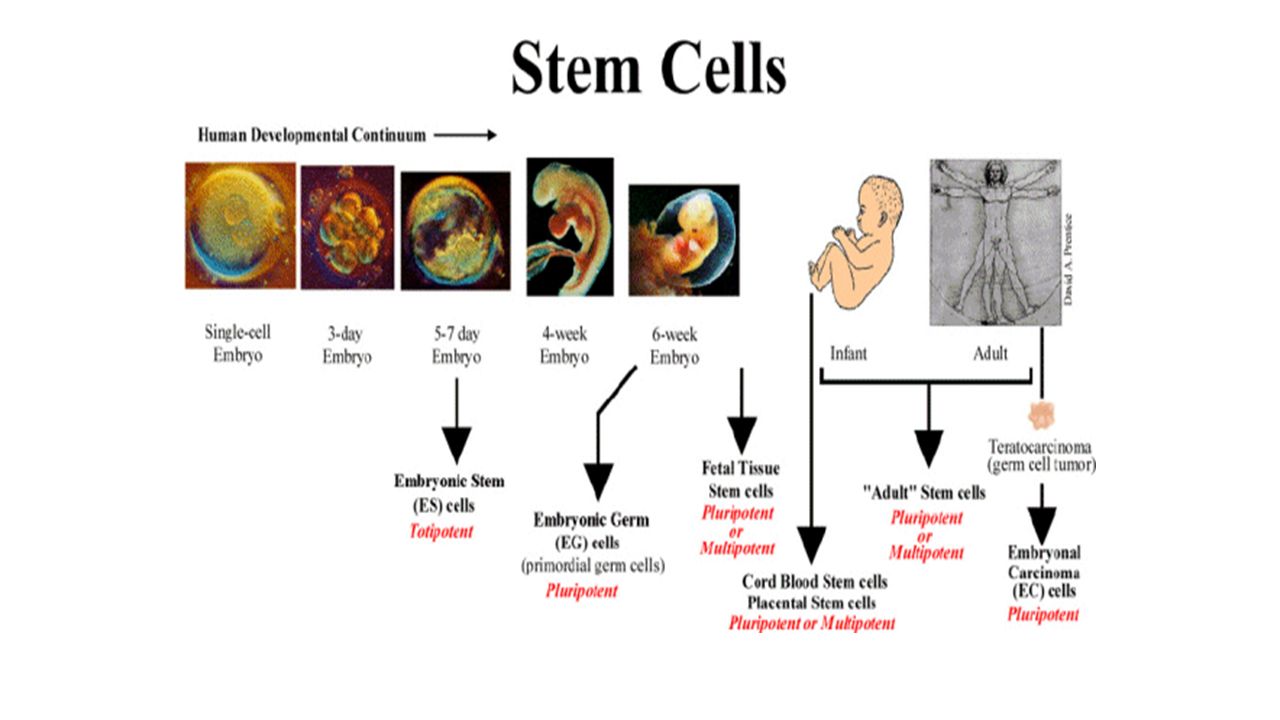
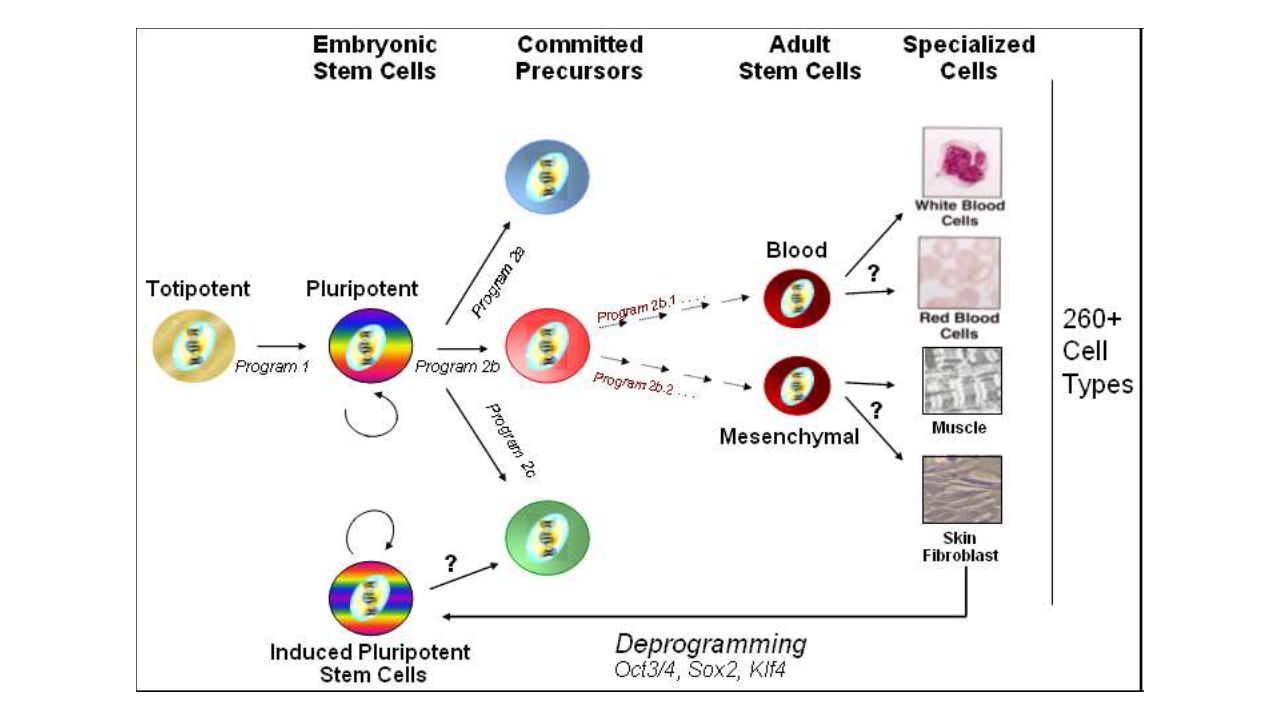
Stem cell jargon PotencyA measure of how many types of specialized cell a stem cell can make PluripotentCan make all types of specialized cells in the body Embryonic stem cells are pluripotent MultipotentCan make multiple types of specialized cells, but not all types Tissue stem cells are multipotent

11
Stem cells: Stem cells: population of undifferentiated cells which are able to divide for indefinite period to self renew to generate a functional progeny of highly specialised cells

12
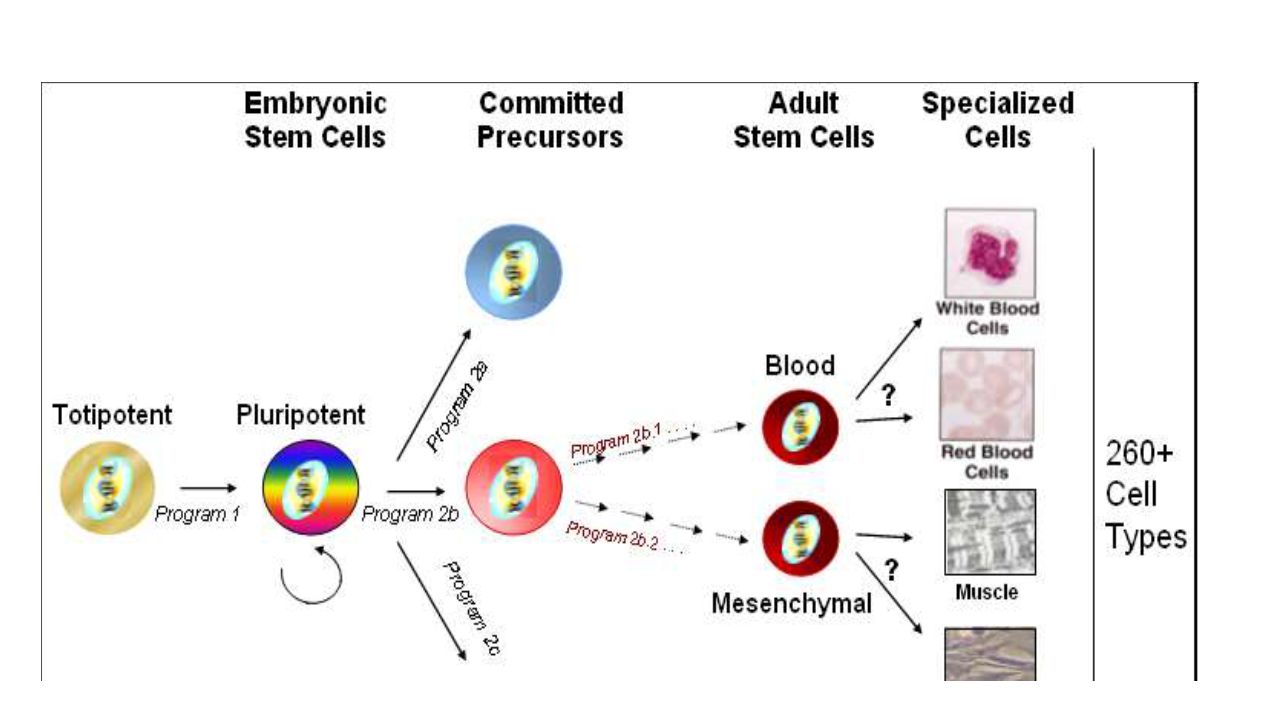
Hierarchy: Totipotent (fertilised egg)Totipotent (fertilised egg) Pluripotent (embryonic cell)Pluripotent (embryonic cell) Multipotent (haematopoietic)Multipotent (haematopoietic)
Totipotent (fertilised egg) Pluripotent (embryonic cell)Pluripotent (embryonic cell) Multipotent (haematopoietic)Multipotent (haematopoietic)")
13
Stem Cell Differentiation

14
Kinds of Stem Cells Stem cell typeDescriptionExamples Totipotent Each cell can develop into a new individual Cells from early (1-3 days) embryos Pluripotent Cells can form any (over 200) cell types Some cells of blastocyst (5 to 14 days) Multipotent Cells differentiated, but can form a number of other tissues Fetal tissue, cord blood, and adult stem cells
 embryos Pluripotent Cells can form any (over 200) cell types Some cells of blastocyst (5 to 14 days) Multipotent Cells differentiated, but can form a number of other tissues Fetal tissue, cord blood, and adult stem cells")
15
Potential of Stem Cells Totipotent (total): Total potential to differentiate into any adult cell type Total potential to form specialized tissue needed for embryonic development Pluripotent (plural): Potential to form most or all 210 differentiated adult cell types Multipotent (multiple): Limited potential Forms only multiple adult cell types Oligodendrocytes Neurons Adult stem cells typically generate the cell types of the tissue in which they reside Stem cells that reside in bone marrow give rise to RBC, WBC and platelets Plasticity Recent experiments have raised the possibility that stem cells from one tissue can give rise to other cell types (Plasticity)
: Total potential to differentiate into any adult cell type Total potential to form specialized tissue needed for embryonic development Pluripotent (plural): Potential to form most or all 210 differentiated adult cell types Multipotent (multiple): Limited potential Forms only multiple adult cell types Oligodendrocytes Neurons Adult stem cells typically generate the cell types of the tissue in which they reside Stem cells that reside in bone marrow give rise to RBC, WBC and platelets Plasticity Recent experiments have raised the possibility that stem cells from one tissue can give rise to other cell types (Plasticity)")
16
Stem Cell: Definition A cell that has the ability to continuously divide & differentiate (develop) into various other kind(s) of cells/tissues ‘Blank cells’ (unspecialized) Capable of dividing & renewing themselves for long periods of time (proliferation and renewal) Have the potential to give rise to specialized cell types (differentiation)
 into various other kind(s) of cells/tissues ‘Blank cells’ (unspecialized) Capable of dividing & renewing themselves for long periods of time (proliferation and renewal) Have the potential to give rise to specialized cell types (differentiation)")
17
stem cell What is a stem cell? stem cell SELF-RENEWAL (copying) specialized cell e.g. muscle cell, nerve cell DIFFERENTIATION (specializing)
.")
18
What is a stem cell? Identical stem cells Stem cell SELF-RENEWAL (copying) Stem cell Specialized cells DIFFERENTIATION (specializing)
 Stem cell Specialized cells DIFFERENTIATION (specializing).")
19
What are stem cells? The body is made up of about 210 different kinds of specialised cells such as muscle cells, nerve cells, fat cells & skin cells All cells in the body come from stem cells A stem cell is a cell that is not yet specialised The process of specialisation is called differentiation Once the differentiation pathway of a stem cell has been decided, it can no longer become another type of cell on its own Adult Stem Cells or Tissue-Specific Stem Cells Fetal Stem Cells Cord Blood Stem Cells Embryonic Stem Cells Induced Pluripotent Stem Cells (iPS Cells)
.")
20
Stem cells can: self-renew to make more stem cells differentiate into a specialised cell type Embryonic stem cells (pluripotent) Stem cells that can become many types of cells in the body are called pluripotent Tissue stem cells (multipotent) Stem cells that can become only a few types of cells are called multipotent Why are stem cells special?
 Stem cells that can become many types of cells in the body are called pluripotent Tissue stem cells (multipotent) Stem cells that can become only a few types of cells are called multipotent Why are stem cells special")
21
A life story…

25
Adult Stem Cell Transplant

26
Tissue stem cells Known as adult stem cells Includes stem cells isolated from fetal and cord blood Reside in most tissues of the body where they are involved in repair and replacement generally very difficult to isolate already used to treat patients (haematological malignancies, diseases of the immune system) Bone marrow Kidney Lung
 Bone marrow Kidney Lung")
27
Adult stem cells

28
Tissue stem cells: What they can do Multipotent blood stem cell found in bone marrow differentiation only specialized types of blood cell: red blood cells, white blood cells, platelets

29
Tissue stem cells: Haematopoietic stem cells (HSCs) HSC committed progenitors neutrophil NK cell erythrocytes dendritic cell platelets megakaryocyte macrophage eosinophil basophil B cell T cell specialized cells bone marrow
 HSC committed progenitors neutrophil NK cell erythrocytes dendritic cell platelets megakaryocyte macrophage eosinophil basophil B cell T cell specialized cells bone marrow")
30
Haematopoietic stem cells 1 / 25 000 - 100 000 of bone marrow cells 1 / 25 000 - 100 000 of bone marrow cells Characteristic: CD34 CD34 CD133 CD133 Lin - Lin - C-kit (CD117) C-kit (CD117) BCRP BCRP Blood, 15 Jan 2004
 C-kit (CD117) BCRP BCRP Blood, 15 Jan 2004")
31
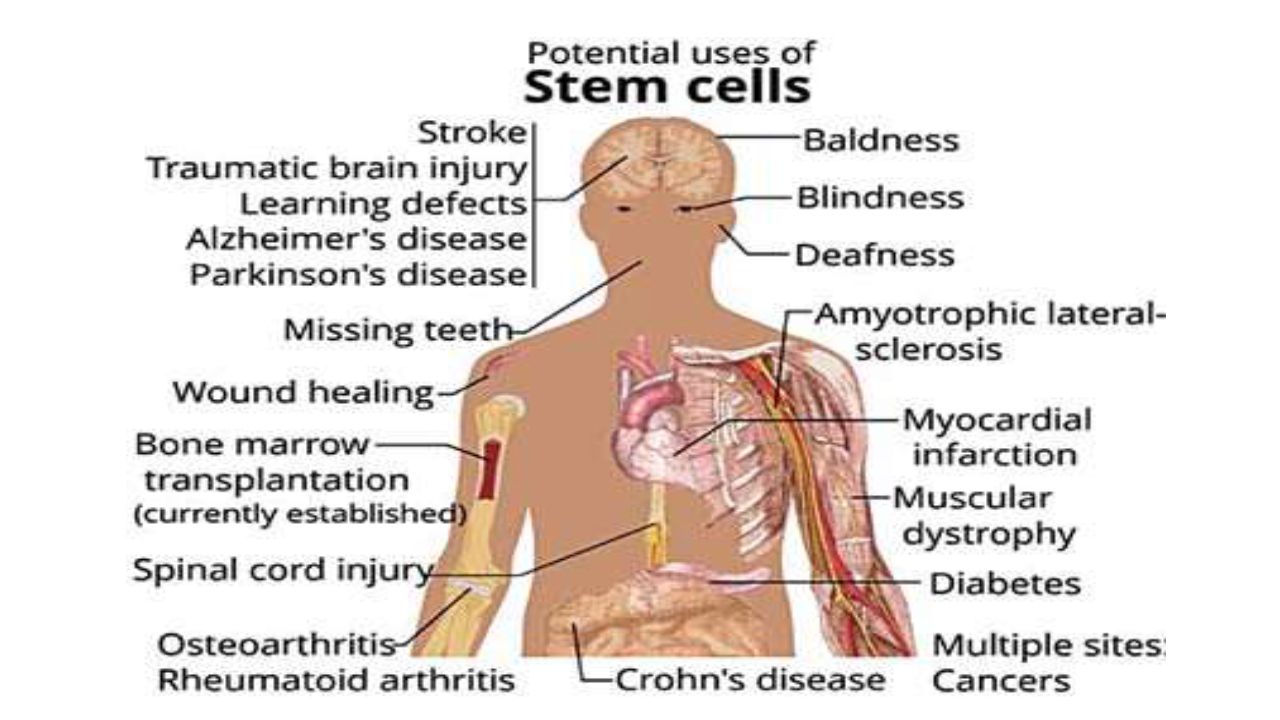
Allo-HSCT: indications AcML, ALL, CML, CLL, MDS, MPN, Multiple myeloma, NHL, HL, AA, PRCA, PNH, Fanconi anaemia, Thalassaemia major, SCA, SCID, Wiskott-Aldrich syndrome, Hemophagocytic lymphohistiocytosis, Inborn errors of metabolism, Epidermolysis bullosa, Severe congenital neutropenia, Shwachman-Diamond syndrome, Diamond-Blackfan anaemia, Leukocyte adhesion deficiency, Osteopetrosis, RA, MG, IDDM, Spinal cord injury Early HSCT-related morbidity & mortality: Mucositis, Haemorrhagic cystitis, Prolonged-severe pancytopenia, Infection, GvHD, Graft failure, Pulmonary complications, Hepatic veno-occlusive disease (VOD or SOS), Thrombotic microangiopathy Late HSCT-related morbidity & mortality Chronic GvHD, Ocular effects, Endocrine effects, Pulmonary effects, Musculoskeletal effects, Neurologic effects, Immune effects, Infection, Congestive heart failure, Subsequent malignancy, Psychological effects
, Thrombotic microangiopathy Late HSCT-related morbidity & mortality Chronic GvHD, Ocular effects, Endocrine effects, Pulmonary effects, Musculoskeletal effects, Neurologic effects, Immune effects, Infection, Congestive heart failure, Subsequent malignancy, Psychological effects")
32
Allogén őssejttranszplantáció indikácói: felnőtt AML AML : közepes és magas rizikó esetén 1. CR-ban (allogén/autológ) Családi donor hiányában magas rizikó esetén MUD donorkeresés javasolt Relabált AML betegek esetén allo-HSCT bármely formája javasolt Idős betegeknél RIC-alloHSCT megfontolandó Primer rezisztens betegségben is javasolt az allo-HSCT bármely formája ALL ALL : magas rizikójú betegek az 1. CR-ban, relabált betegek 2. CR-ban az allo-HSCT bármely donortól CML CML : A Gratwohl és a Sokal pontrendszerek alapján fiatal betegen indokolt a MRD allo- HSCT TKI rezistens eseteknél Idős betegen RIC-alloHSCT megfontolandó CML-AP és CML-BC betegen csak MAC alloHSCT javasolt Egyéb MPN Egyéb MPN : egyéni mérlegelés után kuratív céllal mind MAC mind RIC alloHSCT MDS MDS : allo-HSCT minden formája CLL CLL : magas rizikó esetén RIC-alloHSCT
 Családi donor hiányában magas rizikó esetén MUD donorkeresés javasolt Relabált AML betegek esetén allo-HSCT bármely formája javasolt Idős betegeknél RIC-alloHSCT megfontolandó Primer rezisztens betegségben is javasolt az allo-HSCT bármely formája ALL ALL : magas rizikójú betegek az 1. CR-ban, relabált betegek 2. CR-ban az allo-HSCT bármely donortól CML CML : A Gratwohl és a Sokal pontrendszerek alapján fiatal betegen indokolt a MRD allo- HSCT TKI rezistens eseteknél Idős betegen RIC-alloHSCT megfontolandó CML-AP és CML-BC betegen csak MAC alloHSCT javasolt Egyéb MPN Egyéb MPN : egyéni mérlegelés után kuratív céllal mind MAC mind RIC alloHSCT MDS MDS : allo-HSCT minden formája CLL CLL : magas rizikó esetén RIC-alloHSCT.")
33
: felnőtt Allogén őssejttranszplantáció indikácói: felnőtt HL HL : auto-HSCT relabált betegeknél Primer rezisztens-refracter betegek auto-HSCT javasolt Auto-HSCT után relabáló betegeknél RIC-alloHSCT megfontolandó NHL FL NHL : FL-ban korai relabáló és agresszív klinikai lefolyást mutató esetekben auto- HSCT majd RIC-alloHSCT indokolt DLBCL DLBCL kemoszenzitív relapsusának auto-HSCT javasolt MCL MCL 1. CR-ban auto-HSCT Lymphoblastos lymphomamagas rizikójú Burkit lymphoma Lymphoblastos lymphoma és magas rizikójú Burkit lymphoma 1. CR-ban auto/allo- HSCT T-NHL T-NHL korai intenzifikáció részeként elsősorban az auto-HSCT, de szükséges esetén RIC-alloHSCT is javasolt Myeloma multiplex Myeloma multiplex: ay auto-HSCT 65 (70) év alatt Fiatal myelomás betegeknek az allo-HSCT hozhat végleges gyógyulást
 év alatt Fiatal myelomás betegeknek az allo-HSCT hozhat végleges gyógyulást.")
34
Allogén őssejttranszplantáció indikácói: felnőtt AL amyloidosis AL amyloidosis : súlyos szív és vese érintettség nélküli betegségek auto- HSCT SAA SAA : fiatal betegekben az allo-HSCT (MRD) eredményei jobbak mint az IST. MUD csak 3. vonalban jöhet szóba, ha már két alkalommal történt ATG kezelés eredménytelen PNH PNH : súlyos esetekben allo-HSCT Szolid tumorok Szolid tumorok : extragonadalis germinális sejtes tumorok, Ewing sarcoma, és neuroblasztoma auto-HSCT Autoimmun betegségek Autoimmun betegségek : konzervatív terápiára rezisztens súlyos autóimmun betegségek válogatott esetei (SLE, CIDP, scleroderma, sclerosis multiplex, rheumatoid arthritis, immuncytopeniák, Crohn betegség) auto- HSCT/RIC-alloHSCT
 auto- HSCT/RIC-alloHSCT.")
35
Allogén őssejttranszplantáció indikácói: gyermek AML AML : HLA-identikus családi donor esetében, a magas rizikójú betegek 1. CR esetén (BL kivételével) Egyéb esetekben 2. CR esetén allo-HSCT Amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB HSCT egyedi elbírálás alapján Amennyiben HLA-identikus családi, MUD, nem identikus családi donoros vagy UCB őssejtes donor nem áll rendelkezésre, auo-HSCT egyedi elbírálás alapján ALL ALL : Magas rizikójú betegeknél, valamint t (9;21) és t(4;11) esetekben 1. CR-ban allo-HSCT javasolt A többi betegeknél 2. CR-ban az allo-HSCT CML CML : allo-HSCT egyedi elbírálás alapján HLA-identikus családi donorral vagy amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB NHL NHL : a primer kezelés utáni PR-ban lévő esetben, HLA-identikus családi donor allo-HSCT Amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján 2. CR esetén, HLA-identikus családi donorral vagy MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Amennyiben allo-HSCT nem lehetséges, auto-HSCT javasolt
 Egyéb esetekben 2. CR esetén allo-HSCT Amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB HSCT egyedi elbírálás alapján Amennyiben HLA-identikus családi, MUD, nem identikus családi donoros vagy UCB őssejtes donor nem áll rendelkezésre, auo-HSCT egyedi elbírálás alapján ALL ALL : Magas rizikójú betegeknél, valamint t (9;21) és t(4;11) esetekben 1. CR-ban allo-HSCT javasolt A többi betegeknél 2. CR-ban az allo-HSCT CML CML : allo-HSCT egyedi elbírálás alapján HLA-identikus családi donorral vagy amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB NHL NHL : a primer kezelés utáni PR-ban lévő esetben, HLA-identikus családi donor allo-HSCT Amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján 2. CR esetén, HLA-identikus családi donorral vagy MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Amennyiben allo-HSCT nem lehetséges, auto-HSCT javasolt.")
36
Allogén őssejttranszplantáció indikácói: gyermek HL HL : CR hiánya esetén vagy 2. illetve további recidívában auto-HSCT javasolt MDS MDS : allo-HSCT HLA-identikus családi donorral, MUD, nem identikus családi donoros vagy UCB javasolt SAA SAA : allo-HSCT HLA-identikus családi donorral, amenyiben HLA-identikus családi donor nem áll rendelkezésre, ATG + CsA kezelés eredménytelensége esetén MUD, nem identikus családi donoros vagy UCB Haemoglobinopathiák súlyos formái Haemoglobinopathiák súlyos formái : kielégítő szervfunkciók esetén allo-HSCT HLA-identikus családi donor, és amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Súlyos kombinált immundefektus (SCID) Súlyos kombinált immundefektus (SCID) : allo-HSCT HLA-identikus családi donorral vagy amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB Wiskott Aldrich szindróma (WAS) Wiskott Aldrich szindróma (WAS) : kielégítő szervfunkciók esetén allo- HSCT HLA-identikus családi donor egyedi elbírálás alapján Amennyiben HLA-identikus családi donor nem áll rendelkezésre. MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján
 Súlyos kombinált immundefektus (SCID) : allo-HSCT HLA-identikus családi donorral vagy amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB Wiskott Aldrich szindróma (WAS) Wiskott Aldrich szindróma (WAS) : kielégítő szervfunkciók esetén allo- HSCT HLA-identikus családi donor egyedi elbírálás alapján Amennyiben HLA-identikus családi donor nem áll rendelkezésre. MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján.")
37
Allogén őssejttranszplantáció indikácói: gyermek Súlyos leukocita adhéziós deficientia Súlyos leukocita adhéziós deficientia : kielégítő szervfunkciók esetén allo-HSCT HLA-identikus családi donor, és amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Krónikus granulomatosis Krónikus granulomatosis : allo-HSCT HLA-identikus családi donor egyedi elbírálás alapján, és amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján X kromoszómához kötött lymphoproliferativ syndrome X kromoszómához kötött lymphoproliferativ syndrome : allo-HSCT HLA-identikus családi donor egyedi elbírálás esetén, és amennyiben HLA- identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Chediak Higashi syndrome Chediak Higashi syndrome : allo-HSCT HLA-identikus családi donor egyedi elbírálás alapján

38
Allogén őssejttranszplantáció indikácói: gyermek Osteopetrosis Osteopetrosis : allo-HSCT HLA-identikus családi donor, és amennyiben HLA- identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Súlyos lizoszomális raktározási betegségek Súlyos lizoszomális raktározási betegségek : kielégítő szervfunkciók esetén allo-HSCT HLA-identikus családi donor, és amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB Egyéb tárolási betegségek Egyéb tárolási betegségek : allo-HSCT HLA-identikus családi donorral egyedi elbírálás alapján Amennyiben HLA-identikus családi donor nem áll rendelkezésre, MUD, nem identikus családi donoros vagy UCB egyedi elbírálás alapján Magas rizikójú medulloblastoma/PNET Magas rizikójú medulloblastoma/PNET : auto-HSCT egyedi elbírálás alapján Szolid tumorokban és autoimmun betegségek esetén Szolid tumorokban és autoimmun betegségek esetén : auto-HSCT (kivételes esetekben allo-HSCT autoimmun) egyedi elbírálás alapján
 egyedi elbírálás alapján")
39
HSCT Allogeneic HSCT syngeneic from sibling/related donor from unrelated donor Autologous HSCT Sources of stem cells Bone marrow Peripheral blood Umbilical cord blood Fetus liver Fetus liver

40
Autotransplant

41
Allotransplant

42
Donor típusa HLA identikus testvér vagy egyéb rokon HLA identikus idegen donor HLA nem identikus (pl. haploidentikus rokon) HLA nem identikus idegen donor
 HLA nem identikus idegen donor.")
43
Őssejtforrás Csontvelő Perifériás vér Köldökzsinórvér

44
Perifériás őssejt átültetés előnyei és hátrányai Előny: gyorsabb megtapadás rövidebb aplasia kevesebb szövődmény gyorsabb hazamenetel kisebb költségek ismételt ferezisekkel több sejt gyűjthető graft manipuláció (CD34+ szelekció, T sejt mentesítés) Allogén átültetéseknél a donor számára előnyt jelent, hogy nincs szükség műtétre, ambuláns formában alkalmazható, nagy donor-recipiens testtömeg különbségek esetén is lehetővé teszi a transzplantációt. Hátrány: gyakoribb krónikus graft versus host betegség Same TRM /relapse / LFS More chronic GvHD Donor more SAE for PB donations (significant) more deaths (ns) should be stated in the informed consent Patients: no protection against relapse Should we continue to use PB grafts routinely? ??
 more deaths (ns) should be stated in the informed consent Patients: no protection against relapse Should we continue to use PB grafts routinely. .")
45
Köldökvér őssejtek előnyei és hátrányai Előnyök: több éretlenebb őssejtet tartalmaz lymphocytái kevésbé alloreaktívak kisebb eséllyel közvetít fertőzést (CMV) könnyen nyerhető és gyorsan felhasználható nem szükséges teljes HLA egyezés (az eredmények 1 antigén különbség és teljes HLA egyezés mellett azonosak), ezért nagyobb valószínűséggel találni alkalmas donort Hátrányok: őssejt tartalma korlátozott megtapadás lassabb
 könnyen nyerhető és gyorsan felhasználható nem szükséges teljes HLA egyezés (az eredmények 1 antigén különbség és teljes HLA egyezés mellett azonosak), ezért nagyobb valószínűséggel találni alkalmas donort Hátrányok: őssejt tartalma korlátozott megtapadás lassabb")
46
Transplant Process (6 phases) (1)Harvesting (2)Conditioning (3) Stem cell infusion (4) Neutropenic phase (5) Engraftment phase (6) Post-engraftment period
 (1)Harvesting (2)Conditioning (3) Stem cell infusion (4) Neutropenic phase (5) Engraftment phase (6) Post-engraftment period")
47
Transzplantáció szakaszai Kondicionálás Közvetlen poszttranszplantációs szak aplasia (0-30. nap) Korai poszttranszplantációs szak (30-100. nap) Kései poszttranszplantációs szak (100-365. nap)
 Korai poszttranszplantációs szak ( nap) Kései poszttranszplantációs szak ( nap).")
49
Conditioning regimens Principles „space-making” (controversial) immunosuppression disease eradication Strategy Ablative therapy radio/chemo Reduced intensity therapy radio/chemo Non-myloablative therapy radio/chemo
 immunosuppression disease eradication Strategy Ablative therapy radio/chemo Reduced intensity therapy radio/chemo Non-myloablative therapy radio/chemo")
50
Kondicionáló kezelés Mega chemo-radioterápia Cél: A beteg sejtek elpusztítása A megtapadáshoz szükséges immunszuppresszió A beültetett sejtek csontvelői helyének kialakítása M alignus sejtek elpusztítása Immunszuppresszió (rejectio ) “Hely” a donor vérképzés számára a csontvelői stromában Az őssejtátültetést megelőző emelt dózisú kemo-radioterápiát, mely daganatos betegségekben elsősorban a tumor eradikációját célozza 12 Gy összdózist TBI 4 ülésben, frakcionáltan Myeloablative conditioning (MAC) regimen: TBI doses of ≥500 cGY, single fractionated doses of ≥800 cGY, busulfan doses of >9mg/kg, or melphalan doses of >150 mg/m 2 given as single agents or in combination with other drugs Reduced-intensity conditioning (RIC) regimen: lower doses of TBI, fractionated radiation therapy, busulfan, and melphalan than those used to define a myeloablative conditioning regimen
 Hely a donor vérképzés számára a csontvelői stromában Az őssejtátültetést megelőző emelt dózisú kemo-radioterápiát, mely daganatos betegségekben elsősorban a tumor eradikációját célozza 12 Gy összdózist TBI 4 ülésben, frakcionáltan Myeloablative conditioning (MAC) regimen: TBI doses of ≥500 cGY, single fractionated doses of ≥800 cGY, busulfan doses of >9mg/kg, or melphalan doses of >150 mg/m 2 given as single agents or in combination with other drugs Reduced-intensity conditioning (RIC) regimen: lower doses of TBI, fractionated radiation therapy, busulfan, and melphalan than those used to define a myeloablative conditioning regimen")
51
Conditioning Phase The conditioning period typically lasts 7-10 days The purposes are (by delivery of chemotherapy and/or radiation) to eliminate malignancy to provide immune suppression to prevent rejection of new stem cells create space for the new cells Radiation & chemotherapy agents differ in their abilities to achieve these goals
 to eliminate malignancy to provide immune suppression to prevent rejection of new stem cells create space for the new cells Radiation & chemotherapy agents differ in their abilities to achieve these goals")
52
Stem cell processing & infusion Infusion: 20-60 minutes, varies depending on the volume infused The stem cells may be processed before infusion, if indicated Depletion of T cells can be performed to decrease GvHD Premedication with acetaminophen & diphenhydramine to prevent reaction Infused through a CVL, much like a blood transfusion Anaphylaxis, volume overload, and a (rare) transient GVHD are the major potential complications involved Stem cell products that have been cryopreserved contain dimethyl sulfoxide (DMSO) as a preservative & potentially can cause renal failure, in addition to the unpleasant smell & taste
 transient GVHD are the major potential complications involved Stem cell products that have been cryopreserved contain dimethyl sulfoxide (DMSO) as a preservative & potentially can cause renal failure, in addition to the unpleasant smell & taste")
53
Neutropenic & Engraftment Phases During this period (2-4 wk), the patient essentially has no effective immune system Healing is poor, and the patient is very susceptible to infection Supportive care & empiric antibiotic therapy are the mainstays of successful passage through this phase During engraftment period (several wks), the healing process begins with resolution of mucositis & other lesions acquired Fever begins to subside, and infections often begin to clear The greatest challenges at this time are management of GvHD & prevention of viral infections (especially CMV)
, the patient essentially has no effective immune system Healing is poor, and the patient is very susceptible to infection Supportive care & empiric antibiotic therapy are the mainstays of successful passage through this phase During engraftment period (several wks), the healing process begins with resolution of mucositis & other lesions acquired Fever begins to subside, and infections often begin to clear The greatest challenges at this time are management of GvHD & prevention of viral infections (especially CMV)")
54
Post-engraftment Phase This period lasts for months to years Hallmarks of this phase include the gradual development of tolerance, weaning off of immunosuppression, management of chronic GvHD, and documentation of immune reconstitution If donor cells see the host cells as foreign, the donor cells will attack the host. Skin, gut, and liver most likely to be affected Acute < 100 days after the transplant Chronic > 100 days What are risk factors for GvHD? HLA match/mismatch Lymphocytes in graft Inadequate immune suppression Other???

55
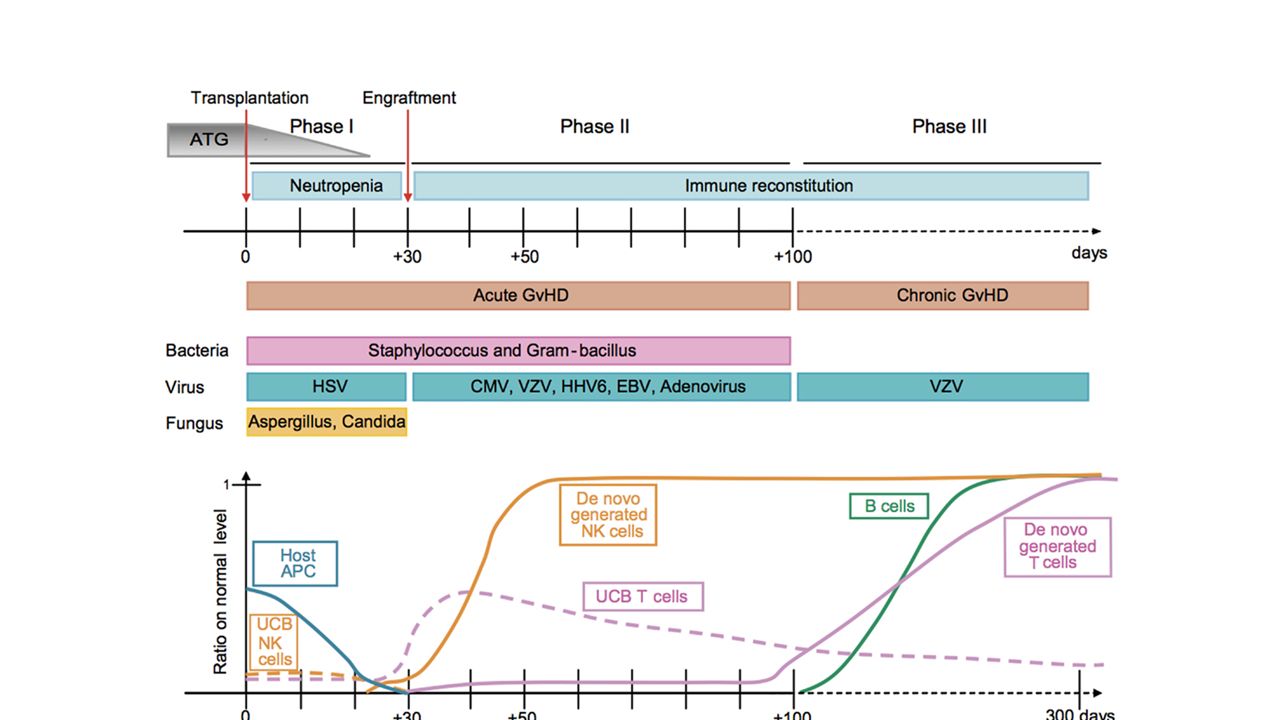
Az immunológiai rekonstitúciót meghatározó tényezők allo-Txp után Transzplantáció: Nincs klinikailag jelentős, tartós donor eredetű T- és B sejt immunválasz-készség A recipiens lympho-haemopoetikus rendszere nagyrészt elpusztult (kondicionálás) A lymphoid rekonstitúció során megismétlődik a lymphoid ontogenesis Transzplantáció előtti tényezők: HLA különbség a donor-recipiens között (MUD, haplo) Recipiens thymus működése (életkor!) A donor és a recipiens korábbi infekciói Transzplantáció jellemzői: Graft T sejt mentesítése (normális IgG termelés 9→12 hónap) Kondicionálás módja („mini”, TBI vagy kemoth.) Anti-lymphocyta antitestek a kondicionálásban Őssejt forrás (periféria vs. csontvelő vs CBU) Transzplantációt követő: Akut és/vagy krónikus GvH (profilaxis és terápia) Fertőzések (elsősorban CMV)
 Transzplantációt követő: Akut és/vagy krónikus GvH (profilaxis és terápia) Fertőzések (elsősorban CMV).")
57
Complications Allogeneic Early infection aGVHD bleeding toxicity graft failure Late chGVHD infection relapse gonadal failure secondary malignancy toxicity Autologous Early infection bleeding toxicity Late relapse infection gonadal failure secondary malignacy toxicity

58
1. fázis: megtapadás előtt 2. fázis: megtapadás után 3. fázis: késői Graft versus host betegség: akut krónikus Neutropenia, Barrierkárosodás (mucositis, centrális kanül) Csökkent humorális és celluláris immunitás; először NK és sejtek jönnek, de korlátozott T sejt repertoár Csökkent humorális és celluláris immunitás; B- és CD4 T sejtszám lassan nő és a repertoár szélesedik Baktérium Vírus Gomba 0. nap15 - 45. nap 100. nap365. nap után Gram negatív baktériumok Gram pozitív baktériumok Gastrointestinális streptococcusok Tokos baktériumok Herpes simplex CMV Varicella zoster Légúti és enterális vírusok Egyéb vírusok: pl. HHV EBV PTLD Aspergillus species Candida species Pneumocystis Ritka Gyakori
 Csökkent humorális és celluláris immunitás; először NK és sejtek jönnek, de korlátozott T sejt repertoár Csökkent humorális és celluláris immunitás; B- és CD4 T sejtszám lassan nő és a repertoár szélesedik Baktérium Vírus Gomba 0. nap nap 100. nap365. nap után Gram negatív baktériumok Gram pozitív baktériumok Gastrointestinális streptococcusok Tokos baktériumok Herpes simplex CMV Varicella zoster Légúti és enterális vírusok Egyéb vírusok: pl. HHV EBV PTLD Aspergillus species Candida species Pneumocystis Ritka Gyakori.")
59
A HSCT szövődményei Fertőzés Vérzés Gyógyszer mellékhatások GvHD Graft rejekció Korai: Gastroenteritis, Mucositis, Hemorrhágiás cystitis, Venoocclusiv (SOS) májbetegség, Haemolysis, Akut GvHD, Fokozott hajszálér permeabilitás, Leukoencephalopáthia, Graftelégtelenség, Fertőzések, Immundefektusok, Intersticiális pneumonitis, Csontvelői elégtelenség Késői: Pszicho-szociális defektusok, Másodlagos malignitás, Krónikus GvHD, Krónikus tüdőbetegség, Autoimmun betegség, Endokrin működési rendellenesség, Cataracta, Növekedési rendellenesség, Infertilitás, Fogászati problémák, Sugár okozta vesegyulladás
 májbetegség, Haemolysis, Akut GvHD, Fokozott hajszálér permeabilitás, Leukoencephalopáthia, Graftelégtelenség, Fertőzések, Immundefektusok, Intersticiális pneumonitis, Csontvelői elégtelenség Késői: Pszicho-szociális defektusok, Másodlagos malignitás, Krónikus GvHD, Krónikus tüdőbetegség, Autoimmun betegség, Endokrin működési rendellenesség, Cataracta, Növekedési rendellenesség, Infertilitás, Fogászati problémák, Sugár okozta vesegyulladás")
60
Késői mellékhatások Krónikus GvHD Immundefektus és fertőzések Légúti és tüdőbetegségek Autoimmun kórképek Neuroendokrin működészavar Növekedési és fejlődési zavar Infertilitás Szívbetegség Szemészeti problémák Mozgásszervi betegségek Fogászati eltérések Húgy-ivarrendszeri működészavarok Gastrointestinális- és májműködési zavarok Malignus betegségek Központi- és perifériás idegrendszeri zavarok Pszichoszociális hatások

61
Krónikus graft versus host betegség (cGvHD)
")
62
Aplasia időszaka (0-30. nap) Neutropenia Thrombocytopenia Anaemia Gyógyszer mellékhatások (haemorrhagiás cystitis, máj-, vesetoxicitás, SOS) Fertőzések (gomba, baktérium, virus) Akut GvHD
 Neutropenia Thrombocytopenia Anaemia Gyógyszer mellékhatások (haemorrhagiás cystitis, máj-, vesetoxicitás, SOS) Fertőzések (gomba, baktérium, virus) Akut GvHD.")
63
A fertőzés helye neutropeniás betegekben Száj-garat Centrális kanül Tüdők Distalis nyelőcső Vastagbél Perianális terület Csontvelő aspiráció helye Orr- és melléküregek

64
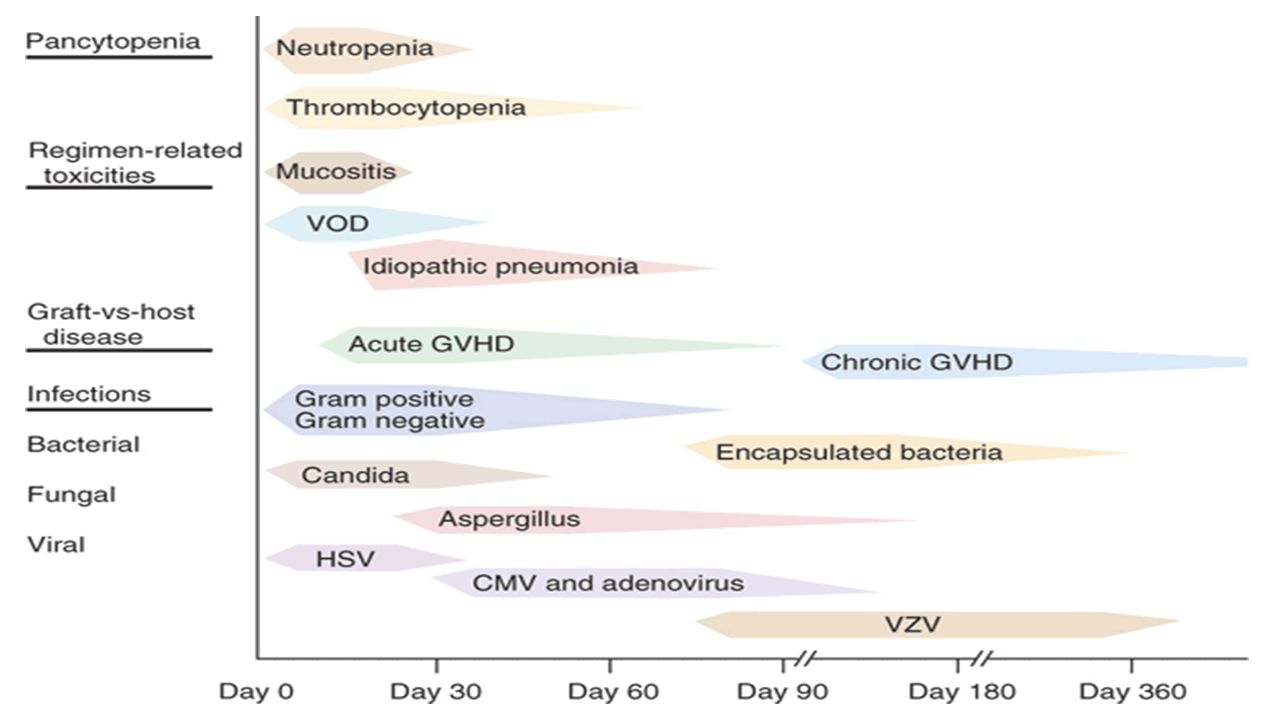
Infekciók allogén HSC-transzplantált betegekben Pneumonia Vírusos Gombás Bakteriális Rizikó tényező Bakteriális HSV Candida Aspergillus Gram poz. Gram neg. Neutropenia Nem bakteriális (intersitialis) CMV Adeno VZV Akut GVHD + Th Krónikus GVHD Ps tokkal bíró baktériumok 0 +50 +10012 Csvt NapokHónapok
 CMV Adeno VZV Akut GVHD + Th Krónikus GVHD Ps tokkal bíró baktériumok Csvt NapokHónapok.")
65
Neutropeniás betegek fertőzéseinek jellegzetességei A gyulladásos jelek és tünetek hiányozhatnak ( duzzanat, erythema, gennyképződés) Mellkas rtg: nincs infiltrátum Meningitis: liquor pleocytosis nélkül Húgyúti fertőzés: pyuria nélkül Haladéktalan, agresszív empirikus kezelés
 Mellkas rtg: nincs infiltrátum Meningitis: liquor pleocytosis nélkül Húgyúti fertőzés: pyuria nélkül Haladéktalan, agresszív empirikus kezelés")
66
Infekció-kontroll Protektív környezet Izolációs technikák: Egyágyas szoba, zsilip, fürdő steril box HEPA-filter túlnyomásos levegőbefúvás 0,5 bar lamináris áramlás Survaillance

67
GvHD Classic acute GvHD: Cases present within 100 days of HSCT & display features of acute GvHD. Diagnostic and distinctive features of chronic GvHD are absent. Persistent, recurrent, late onset acute GvHD: Cases present greater than 100 days post-HSCT with features of acute GvHD. Diagnostic & distinctive features of chronic GvHD are absent. Classic chronic GvHD: Cases may present at any time post-HSCT. Diagnostic & distinctive features of chronic GvHD are present. There are no features of acute GvHD. Overlap syndrome: Cases may present at any time post-HSCT with features of both chronic GvHD & acute GvHD. On occasion, this is colloquially referred to as "acute on chronic" GvHD.

68
Changing Concepts: GvHD Syndrome After Allo-HSCT Day 050100180 1 y2 y 3 y 5 y Acute GVHD: rash, GI, liverChronic GVHD: skin, eyes, mouth, GI liver, musculoskeletal, lungs, GU - Classic acute - Late acute- Classic chronic - Chronic overlap Activity Damage (inflammation) i n j u r y r e p a i r (fibrosis) Alloreactivity Autoimmunity Immunodeficiency All Images Are Copyright Protected
 i n j u r y r e p a i r (fibrosis) Alloreactivity Autoimmunity Immunodeficiency All Images Are Copyright Protected")
69
Risk of GvHD Degree of HLA disparity (HLA mismatch or unrelated donor) Donor & recipient gender disparity (female donor to male recipient) Intensity of the transplant conditioning regimen Acute GvHD prophylactic regimen used Source of graft (peripheral blood or bone marrow greater than umbilical cord blood) Acute GvHD: Skin, GIT, and liver are the principal target organs (rarely haematopoietic, eyes, kidneys) Chronic GvHD: Any organ can be affected
 Donor & recipient gender disparity (female donor to male recipient) Intensity of the transplant conditioning regimen Acute GvHD prophylactic regimen used Source of graft (peripheral blood or bone marrow greater than umbilical cord blood) Acute GvHD: Skin, GIT, and liver are the principal target organs (rarely haematopoietic, eyes, kidneys) Chronic GvHD: Any organ can be affected")
70
Akut Graft versus Host betegség (aGvHD) feltételei A graft immun-kompetens sejteket tartalmazzon A graft és a host alloantigénjei különbözzenek A host ne tudjon hatékony immunválaszt kiváltani a graft ellen (immundeficiens legyen)
 feltételei A graft immun-kompetens sejteket tartalmazzon A graft és a host alloantigénjei különbözzenek A host ne tudjon hatékony immunválaszt kiváltani a graft ellen (immundeficiens legyen)")
71
Alapbetegség Kondicionáló kezelés Egyidejű fertőzés Epithel- és endothelkárosodás Citokin felszabadulás (TNF , IL-1, IFN , GM-CSF, IL-6) Akut graft versus host betegség (aGvHD) MHC II, adhéziós molekulák expressziója: Donor T sejt aktiváció Célsejt apoptosis
 Akut graft versus host betegség (aGvHD) MHC II, adhéziós molekulák expressziója: Donor T sejt aktiváció Célsejt apoptosis")
72
Acute GvHD Skin Skin: Stage 1 - Involvement of less than 25% of the body surface Stage 2 - Involvement of 25-50% of the body surface Stage 3 - Involvement of 50-100% of the body surface (erythroderma) Stage 4 - Vesicles & bullae Histologic staging for acute GVHD is as follows [8] : Grade 0 - Normal skin Grade 1 - Basal cell layer diffuse or focal vacuolar alteration Grade 2 - Grade 1 with epidermis and/or hair follicle dyskeratotic squamous cells Grade 3 - Grade 2 with subepidermal vesicle formation Grade 4 - Complete dermal & epidermal separation
![Acute GvHD Skin Skin: Stage 1 - Involvement of less than 25% of the body surface Stage 2 - Involvement of 25-50% of the body surface Stage 3 - Involvement of % of the body surface (erythroderma) Stage 4 - Vesicles & bullae Histologic staging for acute GVHD is as follows [8] : Grade 0 - Normal skin Grade 1 - Basal cell layer diffuse or focal vacuolar alteration Grade 2 - Grade 1 with epidermis and/or hair follicle dyskeratotic squamous cells Grade 3 - Grade 2 with subepidermal vesicle formation Grade 4 - Complete dermal & epidermal separation](http://images.slideplayer.hu/41/11236187/slides/slide_72.jpg "Acute GvHD Skin Skin: Stage 1 - Involvement of less than 25% of the body surface Stage 2 - Involvement of 25-50% of the body surface Stage 3 - Involvement of % of the body surface (erythroderma) Stage 4 - Vesicles & bullae Histologic staging for acute GVHD is as follows [8] : Grade 0 - Normal skin Grade 1 - Basal cell layer diffuse or focal vacuolar alteration Grade 2 - Grade 1 with epidermis and/or hair follicle dyskeratotic squamous cells Grade 3 - Grade 2 with subepidermal vesicle formation Grade 4 - Complete dermal & epidermal separation")
73
Acute GvHD GIT GIT: Stage 1 – Diarrhea 500 to 1000 mL/day Stage 2 – Diarrhea 1000 to 1500 mL/day Stage 3 – Diarrhea 1500 to 2000 mL/day Stage 4 – Diarrhea >2000 mL/day OR pain OR ileus Liver Liver: Stage 1 – Bilirubin 2 to 3 mg/dL ●Stage 2 – Bilirubin 3 to 6 mg/dL ●Stage 3 – Bilirubin 6 to 15 mg/dL ●Stage 4 – Bilirubin >15 mg/dL

74
Acute GvHD grading The IBMTR grading system defines the severity of acute GvHD as follows: Grade A – Stage 1 skin involvement alone (maculopapular rash over <25 percent of the body) with no liver or GIT involvement Grade B – Stage 2 skin involvement; Stage 1 to 2 gut or liver involvement Grade C – Stage 3 involvement of any organ system (generalized erythroderma; bilirubin 6.1 to 15.0 mg/dL; diarrhea 1500 to 2000 mL/day) Grade D – Stage 4 involvement of any organ system (generalized erythroderma with bullous formation; bilirubin >15 mg/dL; diarrhea >2000 mL/day OR pain OR ileus)
 with no liver or GIT involvement Grade B – Stage 2 skin involvement; Stage 1 to 2 gut or liver involvement Grade C – Stage 3 involvement of any organ system (generalized erythroderma; bilirubin 6.1 to 15.0 mg/dL; diarrhea 1500 to 2000 mL/day) Grade D – Stage 4 involvement of any organ system (generalized erythroderma with bullous formation; bilirubin >15 mg/dL; diarrhea >2000 mL/day OR pain OR ileus)")
75
Couriel et al, Cancer 2004. Acute GvHD of the Skin

76
GvHD of the Skin: Grade IV

77
Treatment of Acute GvHD Primary therapy for acute GvHD: For skin GVHD of stage I or II, observation or a trial of topical corticosteroids (eg, triamcinolone 0.1%) may be used For grade II-IV acute GVHD, continuing the original immunosuppressive prophylaxis and adding methylprednisolone (1-60 mg/kg, most commonly starting at 2 mg/kg/day in 2 divided doses); in patients who respond to initial therapy, short-term tapering treatment with prednisone to a cumulative dose of 2000 mg/m 2 Other therapies are antithymocyte globulin (ATG), cyclosporine alone, mycophenolate mofetil (MMF), daclizumab, anti–IL-2 receptor, anti-CD5–specific immunotoxin, and a pan T-cell ricin A- chain immunotoxin (XomaZyme), alone or in combination Secondary therapy for acute GvHD: ATG or multiple pulses of methylprednisolone (at doses higher than those used in initial therapy) MMF at 2 g daily, added to the steroid regimen Muromomab-CD3 (Orthoclone OKT3) Humanized anti-Tac antibody to the IL-2 receptor Psoralen and ultraviolet A irradiation (PUVA), for cutaneous lesions Tacrolimus, for GVHD with cyclosporine resistance or neurotoxicity
 may be used For grade II-IV acute GVHD, continuing the original immunosuppressive prophylaxis and adding methylprednisolone (1-60 mg/kg, most commonly starting at 2 mg/kg/day in 2 divided doses); in patients who respond to initial therapy, short-term tapering treatment with prednisone to a cumulative dose of 2000 mg/m 2 Other therapies are antithymocyte globulin (ATG), cyclosporine alone, mycophenolate mofetil (MMF), daclizumab, anti–IL-2 receptor, anti-CD5–specific immunotoxin, and a pan T-cell ricin A- chain immunotoxin (XomaZyme), alone or in combination Secondary therapy for acute GvHD: ATG or multiple pulses of methylprednisolone (at doses higher than those used in initial therapy) MMF at 2 g daily, added to the steroid regimen Muromomab-CD3 (Orthoclone OKT3) Humanized anti-Tac antibody to the IL-2 receptor Psoralen and ultraviolet A irradiation (PUVA), for cutaneous lesions Tacrolimus, for GVHD with cyclosporine resistance or neurotoxicity")
78
Chronicus GvHD Kezdetben lichen planusra emlékeztető elváltozások poikiloderma Lokalizált forma: epidermális atrophia, focalis fibrosis, morphea-szerű elváltozások, komoly gyulladás nélkül Generalizált forma: gyulladásos elváltozások kiterjedt fibrosis, scleroderma

79
Lichen planus-like lesions on buccal mucosa showing a lacework of white streaks & erosions Gérard Socié, and Jerome Ritz Blood 2014;124:374-384

80
(A) Lichen planus-like lesions on buccal mucosa showing a lacework of white streaks & erosions (B) Lichen planus lesions of the nails showing thinning of the nail plate, longitudinal lines, and pterygium formation (C) Skin lichen planus lesions with shiny & violaceous papules of the back (D) Edematous erythroderma with lichenoid features evolving into diffuse sclerodermatous changes of the skin
 Lichen planus-like lesions on buccal mucosa showing a lacework of white streaks & erosions (B) Lichen planus lesions of the nails showing thinning of the nail plate, longitudinal lines, and pterygium formation (C) Skin lichen planus lesions with shiny & violaceous papules of the back (D) Edematous erythroderma with lichenoid features evolving into diffuse sclerodermatous changes of the skin")
81
Infections Disability Quality of life Endocrine Metabolism Nutrition Pain Ocular sicca Oral ulcers Nail dystrophy Skin sclerosis Deep sclerosis Bronchiolitis obliterans Loss of bile ducts Fasciitis Skin ulcers Spectrum of manifestations in chronic GvHD

82
GvHD

83
Lichenizált szájnyálkahártya (Krónikus graft versus host betegség)
")
85
Chronic Extensive GvHD

86
Treatment of Chronic GvHD Primary therapy for chronic GvHD: Prednisone, 1 mg/kg every other day Cyclosporine, 6 mg given every 12 hours every other day in patients at high risk for GVHD with thrombocytopenia Thalidomide Secondary therapy for chronic GvHD: MMF, added to standard tacrolimus, cyclosporine, and/or prednisone, for steroid-refractory chronic GVHD Azathioprine, alternating cyclosporine/prednisone, or thalidomide for steroid-refractory chronic GVHD Clofazimine, for treating cutaneous and oral lesions of chronic GVHD and as a steroid-sparing agent PUVA therapy, for refractory cutaneous chronic GVHD Extracorporeal photopheresis (a modification of PUVA treatment) Rituximab, mainly for musculoskeletal and cutaneous chronic GVHD Pentostatin Low-dose (100-cGy) total lymphoid irradiation to thoracoabdominal areas Imatinib
 Rituximab, mainly for musculoskeletal and cutaneous chronic GVHD Pentostatin Low-dose (100-cGy) total lymphoid irradiation to thoracoabdominal areas Imatinib")
87
Conclusions 1.Caution required for donor harvest (BM & especially PB) 2.Several options for HLA /non HLA donor selection 3.Three agents (C+M+other) for appropriate GvHD prophylaxis 4.Time to transplant= crucial factor 5. Should we continue to use PB??

88
Transplant rejection occurs as a result of anti MHC immune responses The MHC was discovered using inbred strains of mice T cells recognise antigens in the context of MHC molecules MHC molecules bind to peptide antigens The structure of MHC molecules is directly related to their function in antigen presentation Polymorphism and polygenism in the MHC protects the population from pathogens evading the immune system Summary

Hasonló előadás