Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Dr. Alföldi Sándor Semmelweis Egyetem, I. Belklinika
A hypertonia, mint a stroke rizikófaktora: fókuszban a szisztolés nyomás Dr. Alföldi Sándor Semmelweis Egyetem, I. Belklinika Budapest,

2
Rokkantságot okozó betegségek sorrendje világszerte (DALY)
1990 Respiratoricus infectiók Diarrhoea Perinatalis kórképek Unipolaris depresszió Ischaemiás szívbetegség Cerebrovascularis kórképek 2020 Ischaemiás szívbetegség Unipolaris depresszió Közúti balesetek Cerebrovascularis kórképek COPD Respiratoricus infectiók Murray & Lopez Lancet 1997;349: and

3
Stroke tények Morbiditás: minden 2. mp-ben 1 stroke
Mortalitás: minden 6. mp-ben 1 stroke halál a második leggyakoribb halálok rendkívülien rontja az életminőséget és a függetlenséget az emberek ezért sokkal jobban félnek a stroke-tól, mint az infarctustól súlyos financiális teher (család, kórház, biztosító)
")
4
Number of Strokes Patients Hospitalised Annually in Europe
Country Number of Strokes Austria 36,596 Belgium 20,000 Croatia 16,259 Denmark 12,500 Estonia ,037 (1st Only) Finland NA France NA Germany 50,000 Greece NA Hungary ,722 Country Number of Strokes Ireland NA Italy NA Israel ,000 Netherlands NA Poland ,000 Portugal ,054 Slovenia ,202 Spain NA Sweden ,000 Turkey ,000 UK ,000 Brainin M, et al., European Journal of Neruology, 2000; 7:5-10.
 Finland NA. France NA. Germany 50,000. Greece NA. Hungary 50,722. Country Number of Strokes. Ireland NA. Italy NA. Israel 13,000. Netherlands NA. Poland 50,000. Portugal 29,054. Slovenia 3,202. Spain NA. Sweden 25,000. Turkey 108,000. UK 130,000. Brainin M, et al., European Journal of Neruology, 2000; 7:5-10.")
5
A stroke-helyzet Magyarországon
Magyarországon az 50 évnél fiatalabb nők 5-ször, a férfiak 6-szor gyakrabban kapnak szélütést évente, mint az EU országok lakosai.2 Az ismételt stroke előfordulási aránya 5 éven belül: %.2 Halálozás: - országos átlag 18,2% - stroke centrumokban 12,1% Ref 1: P.188 Annex Table.2 L.45 Ref 2: P.2 Par.2 S.3 Ref 3: P.17 Par.3 S.7 Ref 4: P.203 Col.1 Par.1 S.6 Ref 5: P.1417 Col.1 Par.1 S.1 Slide 4: The Consequences of Stroke The World Health Organization (WHO) estimates that there were 5.5 million deaths worldwide due to stroke in [Ref 1: P.188 Annex Table.2 L.45] In contrast, another 15 million people worldwide survive minor strokes each year.2 [Ref 2: P.2 Par.2 S.2-3] In the United States, 15 to 30% of people who survive a stroke are permanently disabled.3 [Ref 3: P.17 Par.3 S.7] The consequences of stroke may impact not only the stroke victim but the caregivers and family members as well.4 [Ref 4: P.203 Col.1 Par.1 S.6] In Western countries, stroke is the second most common cause of neurologic disability after Alzheimer’s disease.5 [Ref 5: P.1417 Col.1 Par.1 S.1] References: 1. World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; 2002. 2. American Heart Association. Statistical fact sheet—populations: International cardiovascular disease statistics. Available at: ttp:// Accessed March 4, 2003. 3. American Heart Association. Heart Disease and Stroke Statistics—2003 Update. Dallas, Texas: American Heart Association; Available at: identifier= Accessed February 5, 2003. 4. Wolf PA. Cerebrovascular risk. In: Izzo JL Jr, Black HR, eds. Hypertension Primer: The Essentials of High Blood Pressure. 2nd ed. Dallas, Texas: American Heart Association; 1999: 5. Cerebrovascular Disease. In: Beers MH, Berkow R, eds. The Merck Manual of Diagnosis and Therapy. 17th ed. Whitehouse Station, New Jersey: Merck Research Laboratories; 1999: 1, Agyérbetegségek 6. évf. (különszám): 3-7, 2000. 2. Agyérbetegségek 8. évf. (különszám): 7-9, 2002.
 estimates that there were 5.5 million deaths worldwide due to stroke in [Ref 1: P.188 Annex Table.2 L.45] In contrast, another 15 million people worldwide survive minor strokes each year.2 [Ref 2: P.2 Par.2 S.2-3] In the United States, 15 to 30% of people who survive a stroke are permanently disabled.3 [Ref 3: P.17 Par.3 S.7] The consequences of stroke may impact not only the stroke victim but the caregivers and family members as well.4 [Ref 4: P.203 Col.1 Par.1 S.6] In Western countries, stroke is the second most common cause of neurologic disability after Alzheimer’s disease.5 [Ref 5: P.1417 Col.1 Par.1 S.1] References: 1. World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; American Heart Association. Statistical fact sheet—populations: International cardiovascular disease statistics. Available at: ttp:// Accessed March 4, American Heart Association. Heart Disease and Stroke Statistics—2003 Update. Dallas, Texas: American Heart Association; Available at: identifier= Accessed February 5, Wolf PA. Cerebrovascular risk. In: Izzo JL Jr, Black HR, eds. Hypertension Primer: The Essentials of High Blood Pressure. 2nd ed. Dallas, Texas: American Heart Association; 1999: Cerebrovascular Disease. In: Beers MH, Berkow R, eds. The Merck Manual of Diagnosis and Therapy. 17th ed. Whitehouse Station, New Jersey: Merck Research Laboratories; 1999: , Agyérbetegségek 6. évf. (különszám): 3-7, Agyérbetegségek 8. évf. (különszám): 7-9,")
6
Módositható stroke-rizikófaktorok
Előfordulás % Relatív rizikó Felelős % hypertonia 25-40 hypercholest (>6.2) 6-40 dohányzás 25 inaktivitás elhízás 18 tünetmentes carotis stenosis 2-8 alkoholizmus 2-5 pitvarfibrilláció 1 5 nonvalv 17 valv
 dohányzás inaktivitás elhízás tünetmentes carotis stenosis alkoholizmus pitvarfibrilláció nonvalv 17 valv. 9.")
7
Az atheroscleroticus agyi infarctus rizikófaktorai
Framingham Heart Study - 36-Year Follow-up Kor év Kor év RR RR Ffi Nő Ffi Nő Cholesterol > 240 mg/dL Hypertension > 140/90 mmHg Diabetes ECG-LVH Smoking 1.0 5.7* 3.0+ 5.1* 2.5+ 1.1 4.0* 2.4++ 8.1* 1.0 1.0 2.0* 1.6 3.6* 1.4 1.0 2.6* 2.9* 5.0* 1.9* *p<0.001, + p<0.01, ++ p<0.05 Adv Intern Med 1997; 42:39-66

8
Stroke és hypertonia A stroke betegek 60%-a hypertoniás
Az ismert hypertoniások 30%-a egyáltalán nem, >70%-a nem megfelelően kezelt. A hypertonia növeli a cardioemboliás stroke kockázatát is A pitvarfibrilláló betegek 46 %-a hypertoniás Az összes ischemiás stroke >10 %-a PF eredetű

9
A vérnyomás emelkedése és
a stroke kockázata

10
A stroke mortalitás az életkor és a szisztolés vérnyomás függvényében: 1 millió egyén adatainak meta-analízise Prospective Studies Collaboration, Lancet, 2002;360:1903 40-70 év: > 115/75 Hgmm, +20/10 Hgmm, RRR = 2.0

11
MRFIT: a szisztolés vérnyomás emelkedése nagyobb rizikót jelent, mint a diasztolés
Éves stroke halálozás betegre vetítve 80.6 48.3 43.8 37.4 34.7 38.1 31.0 25.8 24.6 25.3 25.2 24.9 23.8 160+ 16.9 13.9 12.8 12.6 11.8 20.6 10.3 11.8 8.8 8.5 9.2 Szisztolés vérnyomás (Hgmm) <120 100+ 90-99 80-89 75-79 70-74 <70 Diasztolés vérnyomás (Hgmm) Neaton et al. Arch Intern Med, (152) , 1992
 < <70. Diasztolés vérnyomás (Hgmm) Neaton et al. Arch Intern Med, (152) ,")
12
( Kjeldsen,S. et al. Blood Pressure 2001; 10: 190-2 )
Hypertoniás betegeken történt vizsgálatokban a stroke 1990 után már gyakoribb, mint a myocardialis infarctus 1990-ig a gyógyszervizsgálatokban 773 stroke-ot és 1442 akut coronaria syndromát (ACS) jelentettek 37,000 betegben. 1990-óta ismertetett vizsgálatokban 2233 stroke-ot és 1627 ACS-t jelentettek 59,650 betegben. A változás oka ismeretlen. ( Kjeldsen,S. et al. Blood Pressure 2001; 10: )
 jelentettek 37,000 betegben óta ismertetett vizsgálatokban 2233 stroke-ot és 1627 ACS-t jelentettek 59,650 betegben. A változás oka ismeretlen. ( Kjeldsen,S. et al. Blood Pressure 2001; 10: )")
13
Antihypertensiv therapia hatékonysága a stroke preventiojában

14
A gyógyszeres antihipertenzív terápia hatása a szövődményekre
Cerebrovascularis esemény Coronaria betegség Congestiv szívelégtelenség Malignus hypertonia Vese- károsodás Egyéb Előfordulás (%) Modified from Veterans Study 1970; J Am Med Assoc.,
 Modified from Veterans Study 1970; J Am Med Assoc.,")
15
A hypertonia kezelés és a stroke-előfordulás összefüggése
incidencia Kezelt hypertonia Évi incidencia arány főre Hypertonia kezeltségi foka (%) 200 180 140 120 100 80 40 20 160 60 1950- 1954 1955- 1959 1960- 1964 1965- 1969 1970- 1974 1975- 1979 70 50 30 10 Laragh-Brenner, Hypertension
 Laragh-Brenner, Hypertension")
16
Vérnyomás normalizációs rátája
Monoterápiával a betegek mintegy %-ában normalizálható csak a vérnyomás.

17
Systolic vs Diastolic BP Control in Trials on Hypertensives
mmHg mmHg DBP 200 SBP HOPE 120 PROGRESS 190 CAPPP 110 INSIGHT 180 NORDIL 100 170 HOT 160 90 STONE 150 STOP-2 80 140 ALLHAT 130 LIFE 70 B T B T Mancia G., Grassi G., J Hypertension 2002

18
Gyógyszerek száma a célérték eléréséhez
In clinical trials in patients with diabetes or renal impairment randomized to two different BP reduction levels, an average of 3.2 different antihypertensive medications may be needed in order to reach aggressive BP goals in this population.15 The BP average of more aggressively treated patients was slightly less than 140/90 mmHg; these patients experienced much lower rates of cardiovascular events and slower declines in renal function compared to those patients in the higher BP group.15 Slide Reference Bakris GL, Williams M, Dworkin L, et al, for the National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Preserving renal function in adults with hypertension and diabetes: a consensus approach. Am J Kidney Dis. 2000;36: DBP < 85 Hgmm DBP < 75 Hgmm DBP < 80 Hgmm MAP < 92 Hgmm DBP < 85 Hgmm (Reprinted with permission from Bakris GL, et al for the National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis. 2000)
")
19
A hipertónia nem megfelelő beállításának okai
okok a betegek szerint: a gyógyszer hatástalansága túl sok tablettát kell bevenni túl sokszor kell váltogatni a terápiát okok az orvosok szerint: a betegek nem megfelelő complance-e (több, mint 70%)
")
20
Hypertonia és compliance vagy adherence (passzív vagy aktív kapcsolat)
NON-COMPLIANCE OKAI feledékenység (40%), mellékhatás (10%), életmód (10%) A napi egyszeri gyógyszerszedést a betegek 94%-a betartja, a kétszeri szedést csak 78% Jobban tudják gyógyszereik nevét azon betegek, akik otthon rendszeresen mérik vérnyomásukat (55 vs. 33%) Ashida et al: Hyperten., 2000, 23:21-24
, mellékhatás (10%), életmód (10%) A napi egyszeri gyógyszerszedést a betegek 94%-a betartja, a kétszeri szedést csak 78% Jobban tudják gyógyszereik nevét azon betegek, akik otthon rendszeresen mérik vérnyomásukat (55 vs. 33%) Ashida et al: Hyperten., 2000, 23:")
22
SystEur ABPM Substudy: Staessen et al, JAMA. 1999;282:539-546
Az éjszakai-nappali arány és a 24-órás szisztolés átlag önálló cardiovascularis rizikófaktor 10% HR: 1.41 10 mmHg HR: 1.23 SystEur ABPM Substudy: Staessen et al, JAMA. 1999;282:

23
A kora reggeli vérnyomáskiugrás („extrém peaking”) jelentősége a hipertónia kezelésében
D BP -4 -8 -12 mmHg 155 150 * * * 145 * * * * * * * * 140 * * 135 * * 130 Pre-Treatment Post-Treatment 125 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Hours Midnight AM PM p<0,05 at all time points *p=0,0001 (n=111) Adapted from Pickering TG et al., Am J Hypertens, 1994;7:
 Adapted from Pickering TG et al., Am J Hypertens, 1994;7:")
24
A stroke fellépésének cirkadián ritmusa

25
Az excesszív reggeli vérnyomásemelkedés és a stroke
n=519 hypertoniás, idős japán páciens Követés: 4 év MS nem MS 60 20 RRR:39% RRR:62% 19 57 50 * p<0,004 * p<0,001 40 Multiplex cerebralis infarktus prevalenciája (%) 30 35 Stroke (%) 10 20 7,3 10 Az életkor és a 24h szisztolés vérnyomásra történt korrekciót követôen. MS (morning surge): Ébredés utáni 2h átlaga és a legalacsonyabb vérnyomású óra különbsége>55 Hgmm Kario et al., Circulation, márc. 18.
 Stroke (%) , Az életkor és a 24h szisztolés vérnyomásra történt. korrekciót követôen. MS (morning surge): Ébredés utáni 2h átlaga és a legalacsonyabb vérnyomású óra. különbsége>55 Hgmm. Kario et al., Circulation, márc. 18.")
26
A tartós és egyenletes gyógyszerhatás mérőszámai
Az antihipertenziv gyógyszerek teljes intervallumú hatékonyságát mérik: Maradék/csúcshatás (M/Cs): A a kezelés előtti görbéhez viszonyított csúcshatás (Cs) és a következő adag bevételekor még észlelhető maradékhatás (M) aránya. Ideális: 100%, elfogadható >50% Simasági index (SI): gyógyszerek vérnyomás csökkentő hatásának vizsgálata a teljes 24-óra alatt. Számítása: kiszámítjuk a kezelés indukálta átlagos óránkénti vérnyomás csökkenést és annak szórását: SI = H/SDH
: A a kezelés előtti görbéhez viszonyított csúcshatás (Cs) és a következő adag bevételekor még észlelhető maradékhatás (M) aránya. Ideális: 100%, elfogadható >50% Simasági index (SI): gyógyszerek vérnyomás csökkentő hatásának vizsgálata a teljes 24-óra alatt. Számítása: kiszámítjuk a kezelés indukálta átlagos óránkénti vérnyomás csökkenést és annak szórását: SI = H/SDH.")
27
Csúcskoncentráció (h) “First-pass” metabolizmus (%)
Dihidropiridinek farmakokinetikai és farmakodinamikai tulajdonságai Amlodipine 6-12 35-50 65-80 < 5% hatástalan metabolitok 65-85% Nifedipine GITS 5-10 “12-18” 30-60 < 50% hatástalan metabolitok 45-85% Felodipine ER 3-7 “16-22” 15-35 < 65% hatástalan metabolitok 25-50% Lacidipine 1-3 3-8 5-15 < 75% hatástalan metabolitok 35-65% Csúcskoncentráció (h) Felezési idő (h) Biohasznosulás (%) “First-pass” metabolizmus (%) Maradékhatás per csúcshatás (%)
 Felezési idő. (h) Biohasznosulás (%) First-pass metabolizmus (%) Maradékhatás per. csúcshatás (%)")
28
Az egyes antihipertenzív szerek smoothness indexei:
az egyenletes és tarós gyógyszerhatás mértéke Parati G, J Hypertens 2001;19 (suppl2):S174
:S174.")
29
VALUE: A 6. hónapban jól beállított vs nem beállított betegek kockázata
Poolozott kezelési csoportok Esély hányados RRR(%) -25 -45 -21 -14 -36 ** Kardiovaszk. események 0,75 (0,67–0,83) ** Stroke 0,55 (0,46–0,64) ** Összhalálozás 0,79 (0,71–0,88) Myocardialis infarktus 0,86 (0,73–1,01) ** Szívelégtelenség miatti hosp. 0,64 (0,55–0,74) When pooled, the outcomes data indicate that patients who were controlled, regardless of treatment regimen, had significantly better outcomes than those whose blood pressure was not controlled at 6 months.1 Early blood pressure control was a powerful determinant of almost all endpoints (except myocardial infarction).1 1. Weber MA et al. Blood pressure dependent and independent effects of antihypertensive treatment on clinical values in the VALUE trial. Lancet. 2004;363: 0,4 0,6 0,8 1,0 1,2 1,4 Korai jól beállítottak * (n = 10755) Nem-beállított betegek (n = 4490) *sziszt. vérny. < 140 Hgmm a 6. hóban. **p < 0,01. Weber MA et al. Lancet. 2004;363:2047–49.
 ** Kardiovaszk. események. 0,75 (0,67–0,83) ** Stroke. 0,55 (0,46–0,64) ** Összhalálozás. 0,79 (0,71–0,88) Myocardialis infarktus. 0,86 (0,73–1,01) ** Szívelégtelenség miatti hosp. 0,64 (0,55–0,74) When pooled, the outcomes data indicate that patients who were controlled, regardless of treatment regimen, had significantly better outcomes than those whose blood pressure was not controlled at 6 months.1. Early blood pressure control was a powerful determinant of almost all endpoints (except myocardial infarction) Weber MA et al. Blood pressure dependent and independent effects of antihypertensive treatment on clinical values in the VALUE trial. Lancet. 2004;363: ,4. 0,6. 0,8. 1,0. 1,2. 1,4. Korai jól beállítottak * (n = 10755) Nem-beállított betegek. (n = 4490) *sziszt. vérny. < 140 Hgmm a 6. hóban. **p < 0,01. Weber MA et al. Lancet. 2004;363:2047–49.")
30
Weinehall L et al. J Hypertens 2002;20:2081-2088
Vérnyomáskontroll stroke-os betegekben 129 stroke-os beteg közül csak 1-nek jól kontrollált a vérnyomása Weinehall L et al. J Hypertens 2002;20:

31
INVEST A stroke incidenciája és a diastolés vérnyomás

32
Egyformán hatékonyak-e a különböző típusú antihypertensiv szerek?

33
A kalciumantagonista hatás előnyei hypertoniában
A leghatékonyabb antihipertenzív szerek: systolés Önálló natriuretikus, diuretikus hatás Antihypertrophiás hatás (LVH, vasculoprotektív) Antiatherosclerotikus hatás Metabolikus neutralitás Igen jó kombinációs hatékonyság: additiv hatás diuretikummal, potencírozó a többi elsőként választandó antihipertenzív szerrel
 Antiatherosclerotikus hatás. Metabolikus neutralitás. Igen jó kombinációs hatékonyság: additiv hatás diuretikummal, potencírozó a többi elsőként választandó antihipertenzív szerrel.")
34
Az első választásként ajánlott vérnyomáscsökkentők hatékonysági sorrendje
TOMHS VA Neaton et al Meterson et al. Kalciumcsatorna-blokkolók Béta-blokkolók Centrálisan ható szerek ACE-gátlók Thiazid vízhajtók Alfa-blokkolók

35
Az amlodipin vérnyomáscsökkentő hatékonysága
A kiindulási értékkel arányos, dózisfüggő vérnyomáscsökkenés Amlodipin hatása a szisztolés vérnyomásra (Hgmm) Putnam et al. Am J Hypertens (13pt2) 139A, 2000 Calvo et al. Clin Drug Invest (19) , 2000 Grimm et al. Am J Hypertens (13pt2) 134A, 2000 Pitt et al. Circulation (102) , 2000
 Putnam et al. Am J Hypertens (13pt2) 139A, Calvo et al. Clin Drug Invest (19) , Grimm et al. Am J Hypertens (13pt2) 134A, Pitt et al. Circulation (102) ,")
36
A balkamra hypertrophia regressziója

37
Az artériák hypertoniában

38
A kalciumantagonisták vasculoprotectiv hatásai
Antioxidáns hatás2, lipidperoxidáció-gátlás1 Endothel-protektív hatás3 (endothelinszintézis és hatás csökken, NO-termelés nő), apoptosis gátlás4 Thrombocytaaggregáció gátlása5 Simaizom-proliferációt/migrációt gátló hatás7 Atherosclerosis-progressziót gátló hatás8 1Sevanian A et al. Pharm Res 2000 Aug;17(8): Digiesi V. Clin Ter 2000 Jan-Feb;151(1):15-8 3Schiffrin EL. J Hypertens Suppl 1998 Oct;16(5):S Mason RP. J Neurochem 1999 Apr;72(4): 5Chou TC et al. Biochem Pharmacol 1999 Nov 15;58(10): Stepien O. J Cardiovasc Pharmacol 1998 May;31(5):786-93 7Stepien O. Int J Cardiol 1997 Dec 31;62 Suppl 2:S Kramsch DM, Sharma RC. J Hum Hypertens 1995 Mar;9 Suppl 1:S3-9
, apoptosis gátlás4. Thrombocytaaggregáció gátlása5. Simaizom-proliferációt/migrációt gátló hatás7. Atherosclerosis-progressziót gátló hatás8. 1Sevanian A et al. Pharm Res 2000 Aug;17(8): Digiesi V. Clin Ter 2000 Jan-Feb;151(1): Schiffrin EL. J Hypertens Suppl 1998 Oct;16(5):S25-9 4Mason RP. J Neurochem 1999 Apr;72(4): Chou TC et al. Biochem Pharmacol 1999 Nov 15;58(10): Stepien O. J Cardiovasc Pharmacol 1998 May;31(5): Stepien O. Int J Cardiol 1997 Dec 31;62 Suppl 2:S Kramsch DM, Sharma RC. J Hum Hypertens 1995 Mar;9 Suppl 1:S3-9.")
39
WHO-ISH tanulmány Klinikai esemény bekövetkezésének rizikója
ACEi vs placebo CaA vs standard th. CaA Intenzív th. vs enyhébb th. 0.70 0.61 ns 0.86 (1.02) 0.80 0.8 (0.79) borderl. 1.12 heterogen (0.81) 0.81 (0.87) (0.72) (0.82) 0.72 (0.92) 0.85 0.74 (1.04) 0.84 (1.03) Stroke CHD CHF Major CV halálozás Összmort. BPLTTC Lancet 2000; 355:
 (0.79) borderl heterogen. (0.81) (0.87) (0.72) (0.82) (0.92) (1.04) (1.03) Stroke. CHD. CHF. Major. CV. halálozás. Összmort. BPLTTC Lancet 2000; 355:")
40
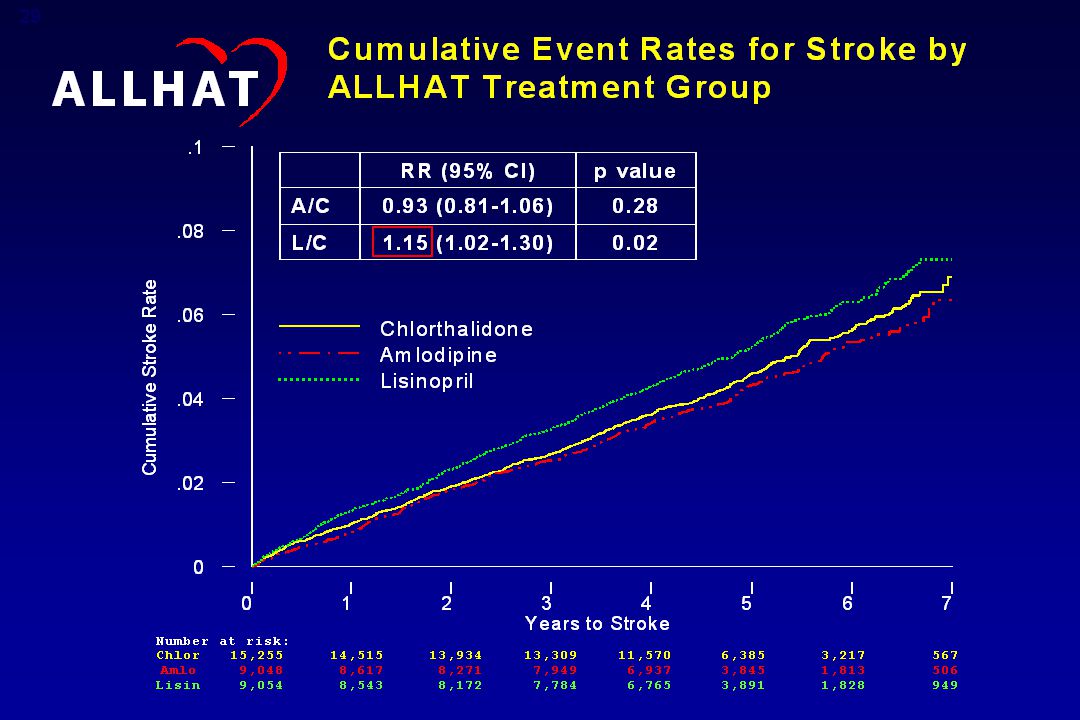
ALLHAT tanulmány 42,448 fokozott kockázatú,
Amlodipin (5-10 mg) +/- Atenolol Chlorthalidon (12,5-25) Reserpin Doxazosin (2-8 mg) Clonidin Lisinopril (10-20 mg) Hydral. Nagy kockázatú hypertoniás betegek Randomizálás kimosás 42,448 fokozott kockázatú, Enyhe-középsúlyos hipertóniás Életkor 55 év Legalább 1 további fő CV morbiditási rizikófaktor
 +/- Atenolol. Chlorthalidon (12,5-25) Reserpin. Doxazosin (2-8 mg) Clonidin. Lisinopril (10-20 mg) Hydral. Nagy kockázatú. hypertoniás. betegek. Randomizálás. kimosás. 42,448 fokozott kockázatú, Enyhe-középsúlyos hipertóniás. Életkor 55 év. Legalább 1 további fő CV morbiditási rizikófaktor.")
42
Az amlodipin besylat indikációja a hipertónia és az angina kezelése.
ALLHAT-vizsgálat: a chlorthalidon és az amlodipin jobban csökkenti a szisztolés vérnyomást a lisinoprilnél 150 a chlorthalidonhoz képest, 5 év alatt Lisinopril Amlodipin Chlorthalidon +2 Hgmm p<0,001 +0,8 Hgmm p=0,03 145 ALLHAT 2002, pp 2987, 2989 Vérnyomás (Hgmm) 140 135 Az ábra az átlagos szisztolés vérnyomásokat mutatja a 3 terápiás csoportban, a 6 évig tartó követés során. A vizsgálat megkezdésekor nem volt jelentős különbség a csoportok között a szisztolés vérnyomást illetően. Az első évre, majd azt követően minden évben, a szisztolés vérnyomások a chlorthalidoncsoportban szignifikánsan alacsonyabbak voltak, mint a lisinopril- vagy amlodipincsoportokban. Az 5. évre a lisinoprilcsoportban a vérnyomás 2 Hgmm-rel magasabb volt, mint a chlorthalidoncsoportban (p<0,001). Az 5. évre, az amlodipincsoportban a vérnyomás 0,8 Hgmm-rel magasabb volt, mint a chlorthalidoncsoportban (p=0,03). ALLHAT 2002, pp 2987, 2989, Fig 2 130 1 2 3 4 5 6 Követés (év) ALLHAT Collaborative Research Group. JAMA. 2002;288: (BP: vérnyomás) The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288: A klinikai vizsgálatokban a placebóhoz viszonyított leggyakoribb mellékhatások az oedema (8,3% vs 2,4%), a fejfájás (7,3% vs 7,8%), a fáradtság (4,5% vs 2,8%) és a szédülés (3,2% vs 3,4%) voltak. Az amlodipin besylat indikációja a hipertónia és az angina kezelése. Kérjük, olvassa el a teljes alkalmazási előiratot is, melyet ez a diasor is tartalmaz. SLIDE 37
 Az ábra az átlagos szisztolés vérnyomásokat mutatja a 3 terápiás csoportban, a 6 évig tartó követés során. A vizsgálat megkezdésekor nem volt jelentős különbség a csoportok között a szisztolés vérnyomást illetően. Az első évre, majd azt követően minden évben, a szisztolés vérnyomások a chlorthalidoncsoportban szignifikánsan alacsonyabbak voltak, mint a lisinopril- vagy amlodipincsoportokban. Az 5. évre a lisinoprilcsoportban a vérnyomás 2 Hgmm-rel magasabb volt, mint a chlorthalidoncsoportban (p<0,001). Az 5. évre, az amlodipincsoportban a vérnyomás 0,8 Hgmm-rel magasabb volt, mint a chlorthalidoncsoportban (p=0,03). ALLHAT 2002, pp 2987, 2989, Fig Követés (év) ALLHAT Collaborative Research Group. JAMA. 2002;288: (BP: vérnyomás) The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288: A klinikai vizsgálatokban a placebóhoz viszonyított leggyakoribb mellékhatások az oedema (8,3% vs 2,4%), a fejfájás (7,3% vs 7,8%), a fáradtság (4,5% vs 2,8%) és a szédülés (3,2% vs 3,4%) voltak. Az amlodipin besylat indikációja a hipertónia és az angina kezelése. Kérjük, olvassa el a teljes alkalmazási előiratot is, melyet ez a diasor is tartalmaz. SLIDE 37.")
43
Carotis IMT amlodipin és lisinopril után
Stanton, Clin Sci 2001; 101:455.

44
LIFE Stroke (fatal and non-fatal)
Atenolol Losartan Percent developing first event Adjusted risk reduction: 24.9%, p=0.0001 Dahlöf B. et al.Lancet 2002

45
A stroke-kockázat csökkenése pitvarfibrillációs betegekben
LIFE Összes stroke 25 Atenolol RRR= - 49% 20 Losartan 15 Betegek első eseménnyel (%) 10 5 Korrigált kockázatcsökkenés 49%, p = 0,018 Ref 1: Poster Col.1 Results Par.2 S.2; Col.1 Conclusion S.2; Fig.1 Slide 21: Reduction in Risk of Stroke in Patients with AF As a predefined subgroup of the LIFE study, the study design was a double-blind, randomized, parallel-group study to evaluate whether Lozartán improves outcomes vs. atenolol in hypertensive patients with ECG-LVH and AF.1 [Ref 1: P.995 Col.1 Par.2 S.1; P.995 Col.2 Par.4 S.4; P.997 T.1 L.3rd from last; Ref 2: Poster Col.1 Background Par.2; Col.1 Methods Par.3] A total of 324 hypertensive patients with ECG-LVH and AF were randomized to receive Lozartán-based or atenolol-based regimens.2 [Ref 2: Poster Col.1 Methods Par.1-2; Col.1 Results S.1] The Kaplan-Meier analysis showed a 49% reduction in risk of stroke in patients receiving Lozartán-based treatment compared with atenolol-based treatment (p = 0.018).2 [Ref 2: Poster Col.1 Results Par.2 S.2; Col.1 Conclusion S.2; Fig.1] The number needed to treat in this subgroup to prevent one stroke was 11 patients.2 [Ref 2: Poster Col.1 Results S.2 + Calculation 3] References: 1. Dalhöf B, Devereux RB, Kjeldsen SE és mtsai, for the LIFE study group. Cardiovascular morbidity and mortality in the Lozartán Intervention For Endpoint reduction in hypertension study (LIFE): A randomised trial against atenolol. Lancet 2002;359: 2. Dalhöf B, Hornestam B, Wachtell K, Aurup P, for the LIFE Study Group. Lozartán decreases the risk of stroke in hypertensive patients with atrial fibrillation and left ventricular hypertrophy. Presented at the European Society of Cardiology Congress; Berlin, Germany; August 31–September 4, Poster 2163. 6 12 18 24 30 36 42 48 54 60 66 Idő (hónapok) Dalhöf B és mtsai. European Society of Cardiology Congress; Berlin, aug. 31. –szept. 4. Poster 2163.
 Korrigált kockázatcsökkenés 49%, p = 0,018. Ref 1: Poster Col.1 Results Par.2 S.2; Col.1 Conclusion S.2; Fig.1. Slide 21: Reduction in Risk of Stroke in Patients with AF. As a predefined subgroup of the LIFE study, the study design was a double-blind, randomized, parallel-group study to evaluate whether Lozartán improves outcomes vs. atenolol in hypertensive patients with ECG-LVH and AF.1 [Ref 1: P.995 Col.1 Par.2 S.1; P.995 Col.2 Par.4 S.4; P.997 T.1 L.3rd from last; Ref 2: Poster Col.1 Background Par.2; Col.1 Methods Par.3] A total of 324 hypertensive patients with ECG-LVH and AF were randomized to receive Lozartán-based or atenolol-based regimens.2 [Ref 2: Poster Col.1 Methods Par.1-2; Col.1 Results S.1] The Kaplan-Meier analysis showed a 49% reduction in risk of stroke in patients receiving Lozartán-based treatment compared with atenolol-based treatment (p = 0.018).2 [Ref 2: Poster Col.1 Results Par.2 S.2; Col.1 Conclusion S.2; Fig.1] The number needed to treat in this subgroup to prevent one stroke was 11 patients.2 [Ref 2: Poster Col.1 Results S.2 + Calculation 3] References: 1. Dalhöf B, Devereux RB, Kjeldsen SE és mtsai, for the LIFE study group. Cardiovascular morbidity and mortality in the Lozartán Intervention For Endpoint reduction in hypertension study (LIFE): A randomised trial against atenolol. Lancet 2002;359: Dalhöf B, Hornestam B, Wachtell K, Aurup P, for the LIFE Study Group. Lozartán decreases the risk of stroke in hypertensive patients with atrial fibrillation and left ventricular hypertrophy. Presented at the European Society of Cardiology Congress; Berlin, Germany; August 31–September 4, Poster Idő (hónapok) Dalhöf B és mtsai. European Society of Cardiology Congress; Berlin, aug. 31. –szept. 4. Poster")
46
Első nagy cardiovascularis esemény gyakorisága a hozzáadott kezelés nélküli betegekben
SCOPE (candesartan vs. placebo) Betegek aránya (%) 16 Vérnyomáscsökkenés különbsége 4,7/2,6 Hgmm 14 Control 12 RR = 32.1% p=0.012 10 8 Candesartan 6 4 2 6 12 18 24 30 36 42 48 54 60 Hónap Cand (n) Control (n)
 Betegek aránya (%) 16. Vérnyomáscsökkenés különbsége 4,7/2,6 Hgmm. 14. Control. 12. RR = 32.1% p= Candesartan Hónap. Cand (n) Control (n)")
47
VALUE: szisztolés vérnyomás a vizsgálatban
Ülve mért szisztolés vérnyomás az idő függvényében, a kezelési csoportokban 155 150 Valsartan (N= 7649) Amlodipin (N = 7596) Hgmm 145 140 135 induláskor 1 2 3 4 6 12 18 24 30 36 42 48 54 60 66 Hónapok (vagy a záróvizitnél) A szisztolés vérnyomás különbségei a valsartan és az amlodipin csoportban 5,0 4,0 3,0 Hgmm At study end (72 months) or final visit, SBP averaged 139.317.6 Hgmm with valsartan-based regimens and 137.515.0 Hgmm with amlodipin-based regimens. The reduction in SBP from baseline until study end was 15.2 Hgmm and 17.3 Hgmm in the valsartan and amlodipin groups, respectively. The difference between groups was substantial at 1 month (4.0 Hgmm) but decreased to approximately 2.1 Hgmm at 6 months and averaged 2.0 Hgmm thereafter. SBP decreased in both treatment groups from 6 months until end of study, by 3.3 Hgmm in the valsartan group and 3.0 Hgmm in the amlodipin group. Control of SBP (<140 Hgmm) was achieved in 58% of the valsartan group and 64% of the amlodipin group by the end of the trial.1 1. Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipin-based regimens: VALUE, a randomised trial. Lancet. 2004;363. 2,0 1,0 1 2 3 4 6 12 18 24 30 36 42 48 54 60 66 –1,0 Hónapok (vagy a záróvizitnél) Julius S et al. Lancet. June 2004;363.
 Amlodipin (N = 7596) Hgmm induláskor Hónapok. (vagy a záróvizitnél) A szisztolés vérnyomás különbségei a valsartan és az amlodipin csoportban. 5,0. 4,0. 3,0. Hgmm. At study end (72 months) or final visit, SBP averaged 139.317.6 Hgmm with valsartan-based regimens and 137.515.0 Hgmm with amlodipin-based regimens. The reduction in SBP from baseline until study end was 15.2 Hgmm and 17.3 Hgmm in the valsartan and amlodipin groups, respectively. The difference between groups was substantial at 1 month (4.0 Hgmm) but decreased to approximately 2.1 Hgmm at 6 months and averaged 2.0 Hgmm thereafter. SBP decreased in both treatment groups from 6 months until end of study, by 3.3 Hgmm in the valsartan group and 3.0 Hgmm in the amlodipin group. Control of SBP (<140 Hgmm) was achieved in 58% of the valsartan group and 64% of the amlodipin group by the end of the trial Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipin-based regimens: VALUE, a randomised trial. Lancet. 2004;363. 2,0. 1, –1,0. Hónapok. (vagy a záróvizitnél) Julius S et al. Lancet. June 2004;363.")
48
Proportion of Patients With First Event (%)
VALUE: halálos és nemhalálos stroke 6 5 4 3 2 1 Valsartan-based regimen Amlodipine-based regimen Proportion of Patients With First Event (%) HR = 1.15; 95% CI = 0.98–1.35; P = 0.08 (NS) There was a trend towards fewer fatal or non-fatal strokes in the amlodipine group, 322 vs 281 in the valsartan and amlodipine groups, respectively (HR=1.15 [95% CI ], P=0.08).1 The Kaplan-Meier curves separated early in favor of amlodipine, and the slopes subsequently became parallel for the remainder of the study.1 1. Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipine-based regimens: VALUE, a randomised trial. Lancet. 2004;363. Time (months) Number at risk Valsartan 7649 7494 7448 7312 7170 7022 6877 6692 6515 6093 3859 1516 Amlodipine 7596 7499 7455 7334 7195 7055 6918 6744 6587 6163 3846 1532 Julius S et al. Lancet. June 2004;363.
 HR = 1.15; 95% CI = 0.98–1.35; P = 0.08 (NS) There was a trend towards fewer fatal or non-fatal strokes in the amlodipine group, 322 vs 281 in the valsartan and amlodipine groups, respectively (HR=1.15 [95% CI ], P=0.08).1 The Kaplan-Meier curves separated early in favor of amlodipine, and the slopes subsequently became parallel for the remainder of the study Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipine-based regimens: VALUE, a randomised trial. Lancet. 2004;363. Time (months) Number at risk. Valsartan Amlodipine Julius S et al. Lancet. June 2004;363.")
49
VALUE: Outcome and SBP Differences at Specific Time Periods: Stroke
Time Interval Δ SBP STROKE (months) (mmHg) Odds Ratios and 95% CIs Overall study 2.2 0–3 3.8 3–6 2.3 6–12 2.0 12–24 1.8 24–36 1.6 36–48 1.4 Study end The association between the greater decrease in SBP with amlodipine and the decrease in stroke was most pronounced in the first 6 months of the trial. As the difference in SPB between groups decreased, so did the odds ratios: in the last 2 years of the study the odds ratio for stroke was lower than unity.1 1. Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipine-based regimens: VALUE, a randomised trial. Lancet. 2004;363. 1.7 0.25 0.5 1.0 2.0 4.0 valsartan előny amlodipin előny Julius S et al. Lancet. June 2004;363.
 (mmHg) Odds Ratios and 95% CIs. Overall study – – – – – – Study end. The association between the greater decrease in SBP with amlodipine and the decrease in stroke was most pronounced in the first 6 months of the trial. As the difference in SPB between groups decreased, so did the odds ratios: in the last 2 years of the study the odds ratio for stroke was lower than unity Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with valsartan- or amlodipine-based regimens: VALUE, a randomised trial. Lancet. 2004; valsartan előny amlodipin előny. Julius S et al. Lancet. June 2004;363.")
50
ASCOT The primary objectives of ASCOT BPLA are: Eligibility criteria:
Nonfatal MI and fatal CHD of a -blocker (atenolol) a diuretic (bendroflumethiazide+K+) with those of a CCB (amlodipine) an ACE (perindopril) Eligibility criteria: Hypertension 40-79 years of age 3+ CVD risk factors The 2 primary objectives of ASCOT are: To compare the effects on the combined outcome of nonfatal MI and fatal CHD of a -blocker (atenolol) a diuretic (bendroflumethiazide+potassium) with those of a CCB (amlodipine) an ACE (perindopril) To compare the effects on the combined outcome of nonfatal MI and fatal CHD of a statin (atorvastatin) with those of placebo in hypertensive patients with TC levels of 6.5 mmol/L (250 mg/dL) Sever PS, et al, for the ASCOT investigators. J Hypertens. 2001;19:
 a diuretic (bendroflumethiazide+K+) with those of a CCB (amlodipine) an ACE (perindopril) Eligibility criteria: Hypertension years of age. 3+ CVD risk factors. The 2 primary objectives of ASCOT are: To compare the effects on the combined outcome of nonfatal MI and fatal CHD of a -blocker (atenolol) a diuretic (bendroflumethiazide+potassium) with those of a CCB (amlodipine) an ACE (perindopril) To compare the effects on the combined outcome of nonfatal MI and fatal CHD of a statin (atorvastatin) with those of placebo in hypertensive patients with TC levels of 6.5 mmol/L (250 mg/dL) Sever PS, et al, for the ASCOT investigators. J Hypertens. 2001;19:")
51
Terápiás protokoll az ASCOT-ban
Antihypertensive arm Lipid-lowering arm Atorvastatin 10 mg/d vs Placebo New Standard Amlodipine Perindopril Doxazosin GITS Atenolol Bendroflumethiazide+K+ Doxazosin GITS The 2x2 factorial design of ASCOT permits the comparison of 2 antihypertensive regimens and a comparison between atorvastatin therapy and placebo. All patients in the trial are randomized to receive antihypertensive therapy, initially with either amlodipine 5 mg/d or atenolol 50 mg/d. In patients who do not achieve a target BP of <140/90 mm Hg (<130/80 mm Hg in patients with diabetes), the dose of amlodipine is titrated to 10 mg/d and the dose of atenolol is titrated to 100 mg/d. In patients who require add-on therapy, amlodipine therapy may be supplemented with (1) perindopril 4-8 mg/d and, if necessary, (2) doxazosin GITS 4-8 mg/d. Atenolol therapy may be supplemented with (1) bendroflumethiazide+potassium mg/d and (2) doxazosin GITS 4-8 mg/d. Patients in the lipid-lowering arm were randomized to receive therapy with atorvastatin 10 mg/d or placebo. Sever PS, et al, for the ASCOT investigators. J Hypertens. 2001;19:
, the dose of amlodipine is titrated to 10 mg/d and the dose of atenolol is titrated to 100 mg/d. In patients who require add-on therapy, amlodipine therapy may be supplemented with (1) perindopril 4-8 mg/d and, if necessary, (2) doxazosin GITS 4-8 mg/d. Atenolol therapy may be supplemented with (1) bendroflumethiazide+potassium mg/d and (2) doxazosin GITS 4-8 mg/d. Patients in the lipid-lowering arm were randomized to receive therapy with atorvastatin 10 mg/d or placebo. Sever PS, et al, for the ASCOT investigators. J Hypertens. 2001;19:")
52
Data Safety Monitoring Board: terminated the study in 3Q 2004
ASCOT BPLA Data Safety Monitoring Board: terminated the study in 3Q 2004 ACC: Preliminary results: Primary endpoint: favours aml/per -13% Stroke: % CV mortality % New onset diabetes -32% Final results: ESC

53
Antihipertenzív kezelés és a dementia
AZ EDDIGI VIZSGÁLATOK ALAPJÁN ÚGY TŰNIK, HOGY: - a DHP CaA (Syst-Eur) - az ARB (LIFE, SCOPE) kezeléssel folytatott antihypertensiv terápia megelőzheti a cognitiv functio romlását, illetve a dementia kialakulását. A thiazid (+BBL?) kezelés ilyen hatását még nem sikerült dokumentálni.
 - az ARB (LIFE, SCOPE) kezeléssel folytatott antihypertensiv terápia. megelőzheti a cognitiv functio romlását, illetve. a dementia kialakulását. A thiazid (+BBL ) kezelés ilyen hatását még nem. sikerült dokumentálni.")
54
„The brain is my second favourite organ”
Woodie Allen

Hasonló előadás