Előadást letölteni
Az előadás letöltése folymat van. Kérjük, várjon

1
Eszméletvesztés-anyagcsere Foglalkozás-egészségügyi
Cseh Károly SE Munka- és Környezet- Egészségtani Tanszék Foglalkozás-egészségügyi Továbbképzés PÁNMED

2
Nem fokális, oldalkülönbség nélkül, normál CT, CSF
Endokrin/metabolikus: hypoglycaemia, ketoacidosis, hyperosmolaris Addison, hypo-, hyperthyreosis hypo-, hyperparathyreosis, Hipofízis elégtelenség

3
In 1921, four scientists at the University of Toronto, Banting, Best, MacLeod, and Collip, first isolated this pancreatic hormone. That year when they published their research in the American Journal of Physiology (Proceedings of the American Physiology Society, December, 1921) they wrote, "we suggest the name insulin." Nine years earlier, Sir Edward Schafer, a noted British physiologist, had suggested in print the existence of the chemical and he had named it insulin, from its secretion in the islets of Langerhans in the pancreas. Even Schafer may have seen a journal article by the French biologist De Meyer who suggested the name insuline in a 1909 publication. Now, did all these separate instances of the word insulin spring up independently, by the merest scientific serendipity, as the result of simultaneous discovery? The progression of publication dates suggests they did not. And Banting, Best, McLeod, and Collip, worthies all, told a small fib. Although diabetics all over the world are grateful for the discovery of insulin, it was a bit tacky of the Ontario scientists to take another man's verbal invention, and try to fob it off as their own creation. To state coyly "we suggest" was tacky , because it suggests that "we" thought up the name. Tacky yes, but typical of a certain persistent brand of University of Toronto arrogance.

4
Best és Banting elso sikeresen kezelt paciense

5
Campbell and Fletcher kezelték a 14 éves Leonard Thompsont.
Banting FG, Best CH, Collip JB, Campbell WR, Fletcher AA. Pancreatic extracts in the treatment of diabetes mellitus. Preliminary report. CMAJ 1922;22(3):141-6. Fletcher AA, Campbell WR: The blood sugar following insulin administration and the symptom complex: hypoglycemia. J Metab Res 2:637– 649, 1922 Campbell and Fletcher kezelték a 14 éves Leonard Thompsont.
: Fletcher AA, Campbell WR: The blood sugar following insulin administration. and the symptom complex: hypoglycemia. J Metab Res 2:637– 649, Campbell and Fletcher kezelték a. 14 éves Leonard Thompsont.")
6
Leonard Thompson Január 11, 1922

7
Teddy Ryder insulinkezelés előtt és után

8
Teddy Ryder egyike volt Banting és Best első pacienseinek.
4 éves korában állapították meg diabetesét. Ez akkor a halálos ítéletét jelentette. Ryder családja hallott a torontói egyetemen folyó munkáról, megkeresték Bantingot. Ryder 1922 nyarától kaphatott insulint - csoda történt ban hunyt el congestiv szívelégtelenségben. Életét szövődményektől mentesen élte le. Túlélte az őt kezelő orvosokat. Az utolsó tanúja volt annak a hőskornak, amelyben az insulinért küzdöttek.

9
Nicolae Paulescu 1916 vizes pancreas extractum, diabeteses kutyának, vércukor csökkenés hormon pancreine

10
George Ludwig Zuelzer (German spelling- Georg Ludwig Zülzer) (April 10, October 16, 1949) German physician, a native of Berlin. Zülzer -diabetes mellitus, pancreatikus kivonat diabeteses kutya, "Acomatrol" haldokló kómás betegnek

11
Sir Edward Sharpey-Schafer (1850-1935) London, 1916
Professor of Physiology University of Edinburgh Ő adta az insuline nevet a hormonnak.

12
Colonel Eli Lilly, Josiah Kirby Lilly Sr., Eli Lilly Jr

13
1876

14
Flush, sápadtság, verejtékezés, nyálfolyás, álmosság, nyugtalanság,
Az 1920-as évek vége: a bécsi pszichiáter, Manfred Joshua Sakel lengyel neurophysiologus Sakel kómát (1927) hozott létre egy alultáplált páciensnél úgy, hogy nagy inzulin- adagokat adott neki, ami hipoglikémiás (abnormálisan alacsony vércukor szint) reakciót és görcsöket okozott. A tanulmányok idegsejt-zsugorodást állapítottak meg és 5%-os halálozási arányt 90 haláleset 12,000 kezelésből E, alkalom, naponta, 2 hónapon át- volt 2 év Flush, sápadtság, verejtékezés, nyálfolyás, álmosság, nyugtalanság, sopor, görcsök, kóma injections were administered six days a week for about two months.[1] The daily insulin dose was gradually increased to units until comas were produced, at which point the dose would be levelled out.[1] Occasionally doses of up 450 units were used.[8] After about 50 or 60 comas, or earlier if the psychiatrist thought that maximum benefit had been achieved, the dose of insulin was rapidly reduced before treatment was stopped.[9][7]Courses of up to 2 years have been documented.[9] After the insulin injection patients would experience various symptoms of decreased blood glucose: flushing, pallor, perspiration, salivation, drowsiness or restlessness.[9]Sopor and coma - if the dose was high enough - would follow.[9]Each coma would last for up to an hour and be terminated by intravenous glucose.[1] Seizures sometimes occurred before or during the coma.[10] Some psychiatrists regarded seizures as therapeutic and patients were sometimes also given electroconvulsive therapy or cardiazol/metrazol convulsive therapy during the coma, or on the day of the week when they didn’t have insulin treatment.[9][10] When they were not in a coma, insulin coma patients were kept together in a group and given special treatment and attention; one handbook for psychiatric nurses, written by British psychiatrist Eric Cunningham Dax, instructs nurses to take their insulin patients out walking and occupy them with games and competitions, flower-picking and map-reading, etc.[11]Patients required continuous supervision as there was a danger of hypoglycaemic aftershocks after the coma.[2] In modified insulin therapy, used in the treatment of neurosis, patients were given lower (sub-coma) doses of insulin.[9]
 hozott létre egy alultáplált páciensnél úgy, hogy nagy inzulin- adagokat adott neki, ami hipoglikémiás (abnormálisan alacsony vércukor szint) reakciót és görcsöket okozott. A tanulmányok idegsejt-zsugorodást állapítottak meg és 5%-os halálozási arányt. 90 haláleset 12,000 kezelésből E, alkalom, naponta, 2 hónapon át- volt 2 év. Flush, sápadtság, verejtékezés, nyálfolyás, álmosság, nyugtalanság, sopor, görcsök, kóma. injections were administered six days a week for about two months.[1] The daily insulin dose was gradually increased to units until comas were produced, at which point the dose would be levelled out.[1] Occasionally doses of up 450 units were used.[8] After about 50 or 60 comas, or earlier if the psychiatrist thought that maximum benefit had been achieved, the dose of insulin was rapidly reduced before treatment was stopped.[9][7]Courses of up to 2 years have been documented.[9] After the insulin injection patients would experience various symptoms of decreased blood glucose: flushing, pallor, perspiration, salivation, drowsiness or restlessness.[9]Sopor and coma - if the dose was high enough - would follow.[9]Each coma would last for up to an hour and be terminated by intravenous glucose.[1] Seizures sometimes occurred before or during the coma.[10] Some psychiatrists regarded seizures as therapeutic and patients were sometimes also given electroconvulsive therapy or cardiazol/metrazol convulsive therapy during the coma, or on the day of the week when they didn’t have insulin treatment.[9][10] When they were not in a coma, insulin coma patients were kept together in a group and given special treatment and attention; one handbook for psychiatric nurses, written by British psychiatrist Eric Cunningham Dax, instructs nurses to take their insulin patients out walking and occupy them with games and competitions, flower-picking and map-reading, etc.[11]Patients required continuous supervision as there was a danger of hypoglycaemic aftershocks after the coma.[2] In modified insulin therapy, used in the treatment of neurosis, patients were given lower (sub-coma) doses of insulin.[9]")
15
Normál vércukor/inzulin ingadozás

16
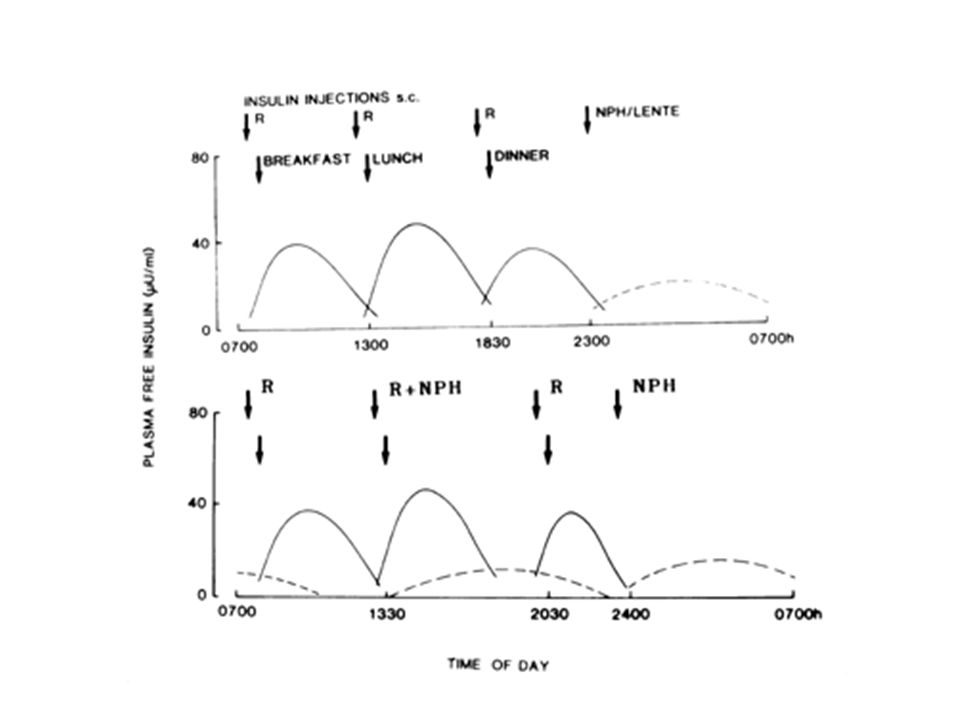
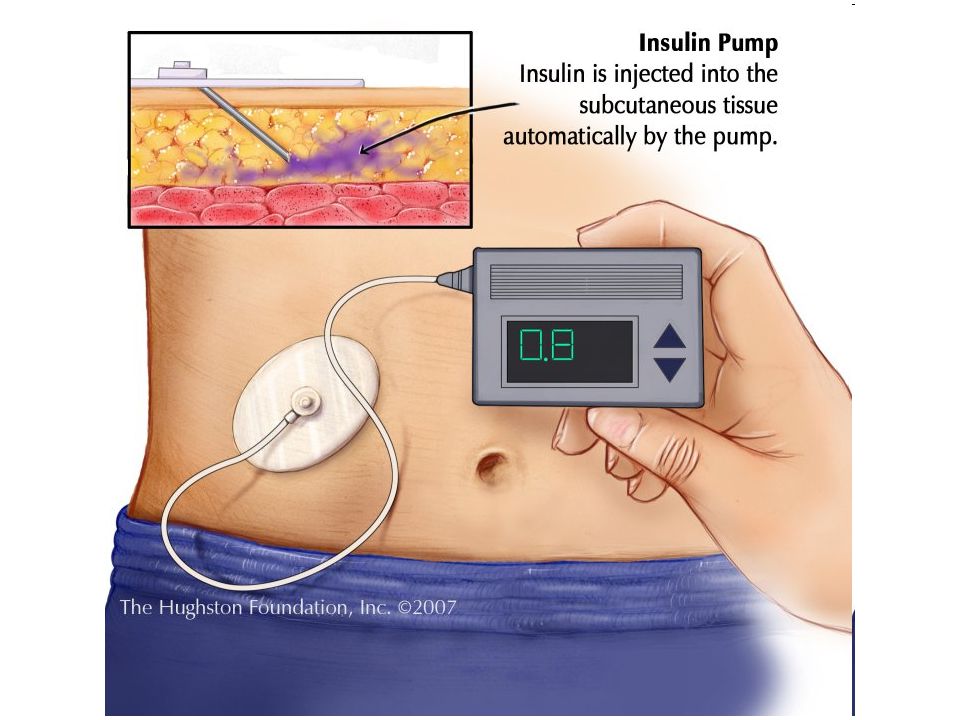
Pharmacokinetics of Insulin Preparations

17
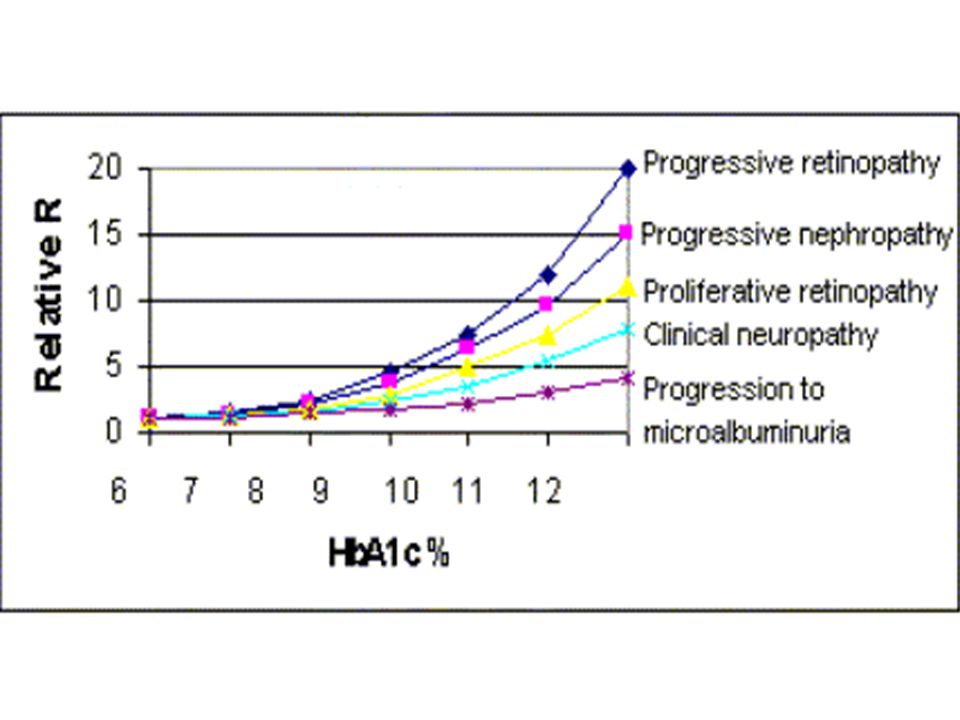
IDF/MDT ADA/EASD Éhomi vc pp HgA1c 7

18
Diabetes Control and Complications Trial (DCCT) 1983-1993
1,441 önkéntes 1DM év USA és Canada 29 centrum The United Kingdom Prospective Diabetes Study (UKPDS) 5,102 beteg 2DM 23 centum, U.K , 10 é RR 140/80 Hgmm alatt Éhomi vc mmol/l HbA1c 7.0% alatt Önellenőrzéses vc étkezés előtt 4-7 mmol/l
 5,102 beteg 2DM 23 centum, U.K , 10 é. RR 140/80 Hgmm alatt Éhomi vc mmol/l HbA1c 7.0% alatt. Önellenőrzéses vc étkezés előtt 4-7 mmol/l")
21
In the Diabetes Control and Complications Trial, there was a progressive increase in the incidence of severe hypoglycemic episodes (per 100 patient-years) at lower attained hemoglobin A1c values during intensive insulin therapy in patients with type 1 diabetes. Data from The Diabetes Control and Complications Trial Research Group, N Engl J Med 1993; 329:977.

22
mg mmol 5 4 3 2 1

23
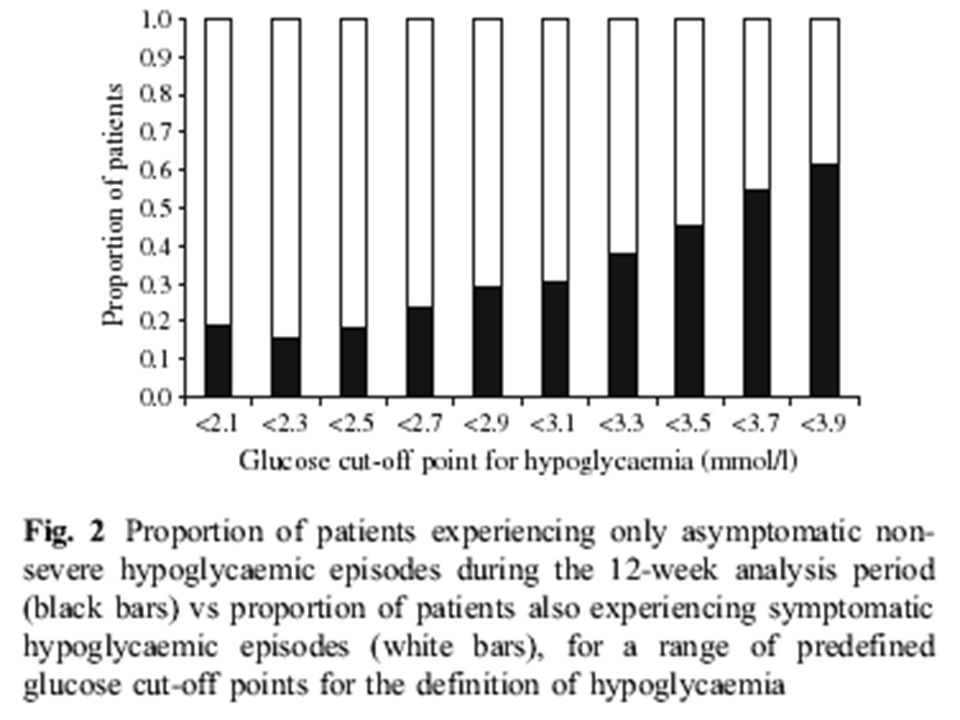
ADA definició <3.9 mmol/l
Hipoglikémia konzervatív definició 4 mmol/l mg/dl (inzulin szekréció gátlás) Klasszikus definició 2.7 mmol/l 50 mg/dl Ellenreguláció (itt kellene észlelni) 3.5 mmol/l mg/dl ADA definició <3.9 mmol/l
 Klasszikus definició. 2.7 mmol/l 50 mg/dl. Ellenreguláció (itt kellene észlelni) 3.5 mmol/l 65 mg/dl. ADA definició <3.9 mmol/l.")
24
3,2 mmol/l alatt autonom és neuroglycopaenias tünetcsoportot,
A vércukorszint 3,8 mmol/l alá csökkenése glucagon és adrenalin felszaporodást, 3,2 mmol/l alatt autonom és neuroglycopaenias tünetcsoportot, 3,0 mmol/l alatt neurofiziológiai dysfunctiot, 2,8 mmol/l alatt kognitiv dysfunctiot, 2,0 mmol/l alatt EEG eltérést, 1,5 mmol/l alatt eszméletlenséget, convulsiokat és halált okozhat. Az Amerikai Diabetes Társaság definícija szerint 3,9 mmol/l alatti vércukorszint alacsonynak számít. Praktikus szempontból azonban 3,l mmol/l-nél alacsonyabb, klinikai tünetekkel járó hypoglycaemiának van gyakorlati jelentősége.

25
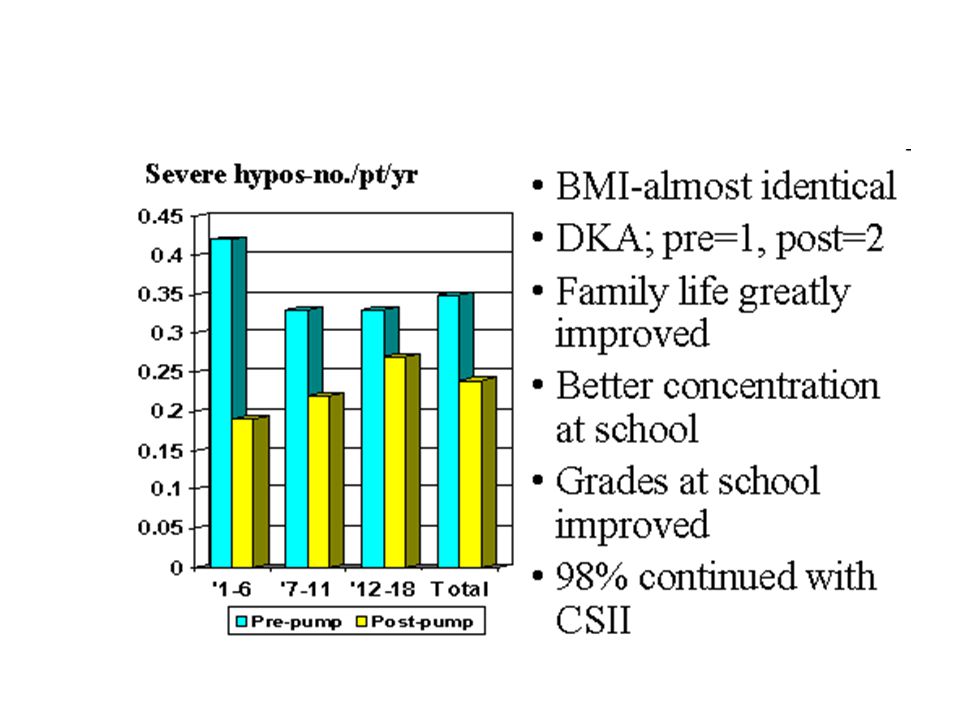
Hipoglikémia prevalencia
1DM intenzív kezelés: 100%, heti 10 szimptómás hipoglikémia évi 1 súlyos, cselekvőképtelenséggel járó 2-4% hipoglikémiával összefüggő halálozás 2DM inzulinkezelés: % Hipoglikémia prediktorok (2DM): inzulin kezelés- megelőző hipoglikémia inzulin kezelés időtartama Megelőző hiperglikémia (magas HbA1c) normál/magasabb vércukor szintnél hipoglikémia tünetcsoport Nőkben kisebb hipoglikémiás válasz Briscoe VJ, Davis SN Clinical Diabetes
: inzulin kezelés- megelőző hipoglikémia. inzulin kezelés időtartama. Megelőző hiperglikémia (magas HbA1c) normál/magasabb. vércukor szintnél hipoglikémia tünetcsoport. Nőkben kisebb hipoglikémiás válasz. Briscoe VJ, Davis SN. Clinical Diabetes")
26
tudatosul nem tudatosul
enyhe súlyos tudatosul nem tudatosul HAAF

27
Hypoglikémia tünetcsoportok
Autonom Neuroglikopéniás Anxietás csökkent kognitív funkciók Idegesség agitáció, emocionális labilitás Remegés melegérzés (hűvös, nedves bőr) Irritabilitás elmosódott látás Émelygés, hányinger elkent beszéd Palpitáció, tachycardia álmosság, szédülés, letargia Verejtékezés confusio Sápadtság apathia Fokozott nyálelválasztás neurológiai deficit (focalis) Pupilla tágulat zavart viselkedés ájulás epileptiform roham
 Irritabilitás elmosódott látás. Émelygés, hányinger elkent beszéd. Palpitáció, tachycardia álmosság, szédülés, letargia. Verejtékezés confusio. Sápadtság apathia. Fokozott nyálelválasztás neurológiai deficit (focalis) Pupilla tágulat zavart viselkedés. ájulás. epileptiform roham.")
28
Glucagon manifestációk (első tünetcsoport?)- 1DM
hypoglycemia 60 or 70 mg/dL (3.3 or 3.9 mmol/L) Glucagon manifestációk (első tünetcsoport?)- 1DM éhség, borborygmus hányinger, hányás, abdominális discomfort fejfájás
 Glucagon manifestációk (első tünetcsoport )- 1DM. éhség, borborygmus. hányinger, hányás, abdominális discomfort. fejfájás.")
29
Geremia B. Bolli How to Ameliorate the Problem of Hypoglycemia in Intensive As Well As Nonintensive Treatment of Type 1 Diabetes Diab Care Volume 22 Supplement 2 B43–B52, 1999

30
Adrenerg manifestációk
bizonytalanság, anxietás, idegesség, tremor Palpitáció, tachycardia verejtékezés, melegérzés sápadtság, hűvös, nyirkos bőr, tág pupillák (mydriasis) érzéketlenség, parasthaesia-tűszúrások
 érzéketlenség, parasthaesia-tűszúrások.")
31
Neuroglikopéniás manifesztációk
Mentális funkciók, csökkent itélőképesség dysphoria, anxietás, hangulati labilitás, depresszió, sírás Negativismus, irritabilitás, ellenségesség, harciasság, düh Személyiség változás, emocionális labilitás kimerültség, gyengeség, apathia, lethargia, révültség, álmosság konfusió, amnézia, szédülés, delirium révülés, „üveges" tekintet, elmosódott látás, kettős látás Automatizmusok Beszédképtelenség, elkent beszéd Ataxia, inkordináció, "részegség látaszata" Focalis vagy generalizált motoros deficit, paralysis, hemiparesis Paresthesia, fejfájás Stupor, coma, légzési zavar Generalizált vagy fokális epilepszia

32
Prandiális Regulátorok (glinid) 1,6
Vércukorcsökkentés Inzulin 4x Sulfanilureák 3x Metformin 1,4 Acarbose 1,2 Tiazolidine dionok 1,4 Prandiális Regulátorok (glinid) 1,6 Hipoglikemizáló
 1,6. Hipoglikemizáló.")
33
Hipoglikémia rizikófaktorok
Kihagyott, késleltetett étkezés Kevesebb szénhidrát bevitele Erőteljes fizikai aktivitás (szénhidrát kompenzáció nélkül Nagyobb adagú inzulin, hipoglikémizáló tbl Alkohol fogyasztás

34
Hipoglikemizáló (gyógy)szerek
Pentamidine Kinin Szalicilátok Szulfonamidok Trimethoprim/sulfometoxasol ketoconasol coumarinok Haloperidol, lithium, triciklikus antidepressansok, klorpromazin, fluoxetin Propoxiphene, stanazol, phenylbutazon Metothrexate, 6-mercaptopurin Insecticidek, carbamatok, organophosphatok Disoprpyramide, propranolol, thiazid diuretikumok, ACE inhibitorok

36
Hajnali jelenség lecseng Fiziológiás IR csökk Tetőzik R
Szinergizál az NPH Risk for preprandial hypoglycemia after subcutaneous injection of a 30/70 insulin mixture of regular/NPH insulin before breakfast in type 1 diabetic patients because of inappropriate hyperinsulinemia in the late morning hours as compared with normal, nondiabetic subjects. Data from Dimitriadis and Gerich (26).
.")
37
cortisol, Adrenalin csökken Vacsora lecseng Bázis inzulin emelkedik IR a legkisebb

38
Sleep, Plasma Glucose, and Epinephrine Concentrations in Five Individuals during Insulin-Induced Hypoglycemia. The panels depict time courses of polysomnographically recorded sleep (black line) in parallel with plasma glucose (green line) and epinephrine (red line) concentrations during the 1-h insulin infusion (0 to 60 min). (A and B) Data from two healthy control participants who displayed the typical awakening response to hypoglycemia. (C) Data from a healthy control participant who did not awaken during hypoglycemia and remained in slow-wave sleep (sleep stages 3 and 4). (D) Data from the only one of the 16 T1DM patients who awakened during hypoglycemia. (E) Data from a typical T1DM patient who did not awaken during hypoglycemia.
 in parallel with plasma glucose (green line) and epinephrine (red line) concentrations during the 1-h insulin infusion (0 to 60 min). (A and B) Data from two healthy control participants who displayed the typical awakening response to hypoglycemia. (C) Data from a healthy control participant who did not awaken during hypoglycemia and remained in slow-wave sleep (sleep stages 3 and 4). (D) Data from the only one of the 16 T1DM patients who awakened during hypoglycemia. (E) Data from a typical T1DM patient who did not awaken during hypoglycemia..")
39
Hipoglikémia-asszociált autonom károsodás (HAAF)
Inzulin szekréció csökkenés Glukagon szekréció fokozódás Adrenomedulláris epinephrin szekréció fokozódás

40
érzékelés szintje csökken
GLUT1 nő Glikogén nő Anyagcsere változás Adrenalin Noradrenalin Acetilkolin

41
Nem tudatosuló hipoglikémia
HbA1c kisebb 6% Nincs autonom tünet <3 mmol/l vércukorszintnél DCCT HbA1C 9% % 300%-os súlyos hypoglikémia növekedés

43
Blood glucose awareness training
3 hetes hipoglikémia elkerülés javít Cox DJ. Diab care 24/

48
Nem tudatosuló hypoglikémia
Csökken LABA hosszúhatású béta agonisták- terbutaline Alanine Methylxantinok- theophyllin, coffein, theobromine Fokozódik SSRI- fluoxetine, sertraline, paroxetine

49
Hipoglikémiás neuronális károsodás
Glutamát receptor aktiváció NADPH oxidáz aktiváció Zinc transzlokáció NO superoxid PARP-1 aktiváció Mitokondriális permeábilitás változás Sequential release of nitric oxide, zinc, and superoxide in hypoglycemic neuronal death. Suh SV et al. Journal of Cerebral Blood Flow & Metabolism (2008) 28, 1697–1706
 28, 1697–1706.")
50
gyrus dentatus memoria, neurogenezis, stress, depresszió
The dentate gyrus is part of the hippocampal formation. It is thought to contribute to new memories as well as other functional roles.[1][2] It is notable as being one of a select few brain structures currently known to have high rates of neurogenesis in adult humans,[3] (other sites include the olfactory bulb and cerebellum).[4][5] The dentate gyrus consists of three layers of neurons: molecular, granular, and polymorphic. The middle layer is most prominent and contains granule cells that project to the CA3 subfield of the hippocampus.[6] These granule cells project mostly to interneurons, but also to pyramidal cells and are the principal excitatory neurons of the dentate gyrus. The major input to the dentate gyrus (the so-called perforant pathway) is from layer 2 of the entorhinal cortex, and the dentate gyrus receives no direct inputs from other cortical structures. The perforant pathway is divided into the medial perforant path and the lateral perforant path, generated, respectively, at the medial and lateral portions of the entorhinal cortex. The medial perforant path synapses onto the proximal dendritic area of the granule cells, whereas the lateral perforant path does so onto the distal dendrites of these same cells. [edit] Function Phenotypes of proliferating cells in the dentate gyrus. A fragment of an illustration from Faiz et al., 2005.[7] The dentate gyrus is thought to contribute to the formation of memories and to play a role in depression. [edit] Memory The dentate gyrus is one of the few regions of the adult brain where neurogenesis (i.e., the birth of new neurons) takes place. Neurogenesis is thought to play a role in the formation of new memories. New memories could preferentially utilize newly-formed dentate gyrus cell, providing a potential mechanism for distinguishing multiple instances of similar events or multiple visits to the same location.[citation needed] [edit] Stress and Depression The dentate gyrus may also have a functional role in stress and depression. For instance, neurogenesis has been found to increase in response to chronic treatment with antidepressants[8]. On the contrary, however, the physiological effects of stress, often characterized by release of glucocorticoids such as cortisol, as well as activation of the sympathetic division of the autonomic nervous system, have been shown to inhibit the process of neurogenesis in primates[9]. Both endogenous and exogenous glucocorticoids are known to cause psychosis and depression,[10], implying that neurogenesis in the dentate gyrus may play an important role in modulating symptoms of stress and depression. [edit] Other Some evidence suggests that neurogenesis in the dentate gyrus increases in response to aerobic exercise[11]. [edit] Blood Sugar Studies by researchers at Columbia University Medical Center indicate that poor glucose control can lead to deleterious effects on the dentate gyrus.[12] memoria, neurogenezis, stress, depresszió 30 min, asszimetria EEG isoelectricitás Dendrit duzzadás
.[4][5] The dentate gyrus consists of three layers of neurons: molecular, granular, and polymorphic. The middle layer is most prominent and contains granule cells that project to the CA3 subfield of the hippocampus.[6] These granule cells project mostly to interneurons, but also to pyramidal cells and are the principal excitatory neurons of the dentate gyrus. The major input to the dentate gyrus (the so-called perforant pathway) is from layer 2 of the entorhinal cortex, and the dentate gyrus receives no direct inputs from other cortical structures. The perforant pathway is divided into the medial perforant path and the lateral perforant path, generated, respectively, at the medial and lateral portions of the entorhinal cortex. The medial perforant path synapses onto the proximal dendritic area of the granule cells, whereas the lateral perforant path does so onto the distal dendrites of these same cells. [edit] Function. Phenotypes of proliferating cells in the dentate gyrus. A fragment of an illustration from Faiz et al., 2005.[7] The dentate gyrus is thought to contribute to the formation of memories and to play a role in depression. [edit] Memory. The dentate gyrus is one of the few regions of the adult brain where neurogenesis (i.e., the birth of new neurons) takes place. Neurogenesis is thought to play a role in the formation of new memories. New memories could preferentially utilize newly-formed dentate gyrus cell, providing a potential mechanism for distinguishing multiple instances of similar events or multiple visits to the same location.[citation needed] [edit] Stress and Depression. The dentate gyrus may also have a functional role in stress and depression. For instance, neurogenesis has been found to increase in response to chronic treatment with antidepressants[8]. On the contrary, however, the physiological effects of stress, often characterized by release of glucocorticoids such as cortisol, as well as activation of the sympathetic division of the autonomic nervous system, have been shown to inhibit the process of neurogenesis in primates[9]. Both endogenous and exogenous glucocorticoids are known to cause psychosis and depression,[10], implying that neurogenesis in the dentate gyrus may play an important role in modulating symptoms of stress and depression. [edit] Other. Some evidence suggests that neurogenesis in the dentate gyrus increases in response to aerobic exercise[11]. [edit] Blood Sugar. Studies by researchers at Columbia University Medical Center indicate that poor glucose control can lead to deleterious effects on the dentate gyrus.[12] memoria, neurogenezis, stress, depresszió. 30 min, asszimetria. EEG isoelectricitás. Dendrit duzzadás.")
51
vérzések hiánya thalamus lézió jeleinek hiánya
Fujioka M et al Specific Changes in Human Brain After Hypoglycemic Injury Stroke. 1997;28: vérzések hiánya thalamus lézió jeleinek hiánya CT bilateralis occipitalis és parietalis corticex MRI bilateral caudate, lenticular nuclei, cerebral cortices, substantia nigra, bilateral hippocampus

52
CT day 10 (A, B) lesions in the bilateral occipital and parietal cerebral cortices
MR days 18 (C, D, E, F, G) 50 (H, I, J, K, L) persistent hyperintense, hypointense lesions T1-weighted (C, E, G, H, I, K) and T2-weighted (D, F, J, L) the bilateral caudate, lenticular nuclei, cerebral cortices (E, G, H; arrows), substantia nigra (K, L; arrows) bilateral hippocampus (C, D, G, K, L). Fujioka, M. et al. Stroke 1997;28: Copyright ©1997 American Heart Association
 50 (H, I, J, K, L) persistent hyperintense, hypointense lesions. T1-weighted (C, E, G, H, I, K) and T2-weighted (D, F, J, L) the bilateral caudate, lenticular. nuclei, cerebral cortices (E, G, H; arrows), substantia nigra (K, L; arrows) bilateral hippocampus. (C, D, G, K, L). Fujioka, M. et al. Stroke 1997;28: Copyright ©1997 American Heart Association.")
53
MRI: bilateral basal ganglia, cerebral cortex, substantia nigra, and hippocampus
Specific changes with time on MRI; serial changes on high-field MR images in each patient. These specific changes in the bilateral basal ganglia, cerebral cortex, substantia nigra, and hippocampus are considered to reflect tissue degeneration, including some combination of selective neuronal death, proliferation of astrocytic glial cells, paramagnetic substance deposition, and/or lipid accumulation but not infarct (pannecrosis) or hemorrhage. T1WI indicates T1-weighted image; T2WI, T2-weighted image. Fujioka, M. et al. Stroke 1997;28: Copyright ©1997 American Heart Association
 or hemorrhage. T1WI indicates T1-weighted image; T2WI, T2-weighted image. Fujioka, M. et al. Stroke 1997;28: Copyright ©1997 American Heart Association.")
54
Table 1. Clinical Features of Four Patients With Transient Profound Hypoglycemia
Pt Agey Sex DM Cause Duration, h BG, mmol/L SLDL CE Outcome 1 58 M Insulin 9 0.56 Cau, Len (day 14) Cau, Len, Cor (days 15-25) PVS 2 85 Glib, poor appetite 8 Ud No SLDL Cor (days 10-23) 3 62 9.5 0.83 Len (day 7) Cau, Len, Cor (days 7-26) 4 63 F Glib, diet 11 Cau, Len (day 9) Cau, Len, Cor (days 12-30) Pt indicates patient; DM, diabetes mellitus; Type 1, insulin-dependent DM; Type 2, noninsulin-dependent DM; BG, blood glucose level on admission; SLDL, symmetrical low-dense lesions; CE, transient contrast-enhanced lesions; Glib, glibenclamide; Cau, caudate nuclei; Len, lenticular nuclei; PVS, persistent vegetative state.
 Cau, Len, Cor (days 15-25) PVS Glib, poor appetite. 8. Ud. No SLDL. Cor (days 10-23) Len (day 7) Cau, Len, Cor (days 7-26) F. Glib, diet. 11. Cau, Len (day 9) Cau, Len, Cor (days 12-30) Pt indicates patient; DM, diabetes mellitus; Type 1, insulin-dependent DM; Type 2, noninsulin-dependent DM; BG, blood glucose level on admission; SLDL, symmetrical low-dense lesions; CE, transient contrast-enhanced lesions; Glib, glibenclamide; Cau, caudate nuclei; Len, lenticular nuclei; PVS, persistent vegetative state.")
55
Journal of Clinical Neuroscience 13 (2006) 696–699
Brain MRI, diffusion weighted images 5 days after presentation. There are diffuse high-intensity signals in the cortex, presumably sparing the motor and sensory centers. 50 days after presentation. The high-intensity signals in the cortex and basal ganglia have resolved. Marked cerebral atrophy is seenThree months later, she remained totally dependent due to aphasia, agnosia and apraxia, but had a normal gait without pyramidal tract signs or ataxia. She remains unchanged 10 months after presentation. A 20-year-old woman was transferred unconsciousness to our hospital by ambulance. Her past medical history included a suicide attempt by drug overdose at 17 years of age when she was pregnant which resulted in an artificial abortion. Her mother suffers from diabetes mellitus and stroke from mitochondrial encephalomyopathy and the patient administered her daily insulin. She was also aware that she had the mitochondrial 3243 mutation, similar to her mother. On examination, there was no eye-opening or verbal response, and her posture was decorticate on painful stimulation, (Glasgow Coma Scale score 5). Her blood pressure was 151/110 mmHg; pulse 168 beats per min; tympanic temperature 35.9 °C; and respiratory rate 24 breaths per min. She had isocoric, reactive pupils and ocular bobbing. The remainder of her examination was normal. Arterial blood gas on 6 liters of oxygen by mask revealed pH 7.39, PCO2 38 mmHg, PO2 442 mmHg, base excess −4.0 mmol/L. Her blood glucose was 17 mg/dL and she was immediately infused with 40 ml of 50% glucose to reach 120 mg/dL. A complete blood count showed white blood cells 3200/mm3, red blood cells 423 × 104/mm3 and platelets 41.9 × 104/mm3. Serum biochemistry revealed total bilirubin 0.6 mg/dL, aspartate aminotransferase 26 international units (IU)/L, alanine aminotransferase 12 IU/L, blood urea nitrogen 6 mg/dL, creatinine 0.3 mg/dL, creatine phosphokinase 102 IU/L, sodium 140 mEq/L, potassium 5.0 mEq/L, chloride 99 mEq/L, ammonia 23 mg/dL. A urinary pregnancy test was positive. Cerebrospinal fluid (CSF) analysis showed crystal clear CSF, initial pressure 20 cmH2O and normal cell count, lactate and pyruvate. A computed tomographic scan of her head demonstrated diffuse brain swelling. An electroencephalogram showed low voltage fast waves and no typical epileptic discharges. Abdominal sonography demonstrated a 10-week-old embryo. She was intubated and ventilated in the intensive care unit and brain swelling and raised intracranial pressure was managed with diuresis. Blood glucose was repeatedly low for the first 12 hours, so she received a continuous glucose infusion. After the second hospital day, she was no longer hypoglycemic. On the third hospital day, serum biochemistry revealed insulin 12.5 μU/mL (<17), c-peptide 0.56 ng/mL (0.94–2.80), free T pg/mL (2.47–4.34), free T ng/mL (0.97–1.79), cortisol 20.2 μg/dL. As she had a past history of suicide attempt, clinical features of temporary hypoglycemia, normal endocrine function including insulin, normal lactate and pyruvate in the CSF, and no hypotension or hypoxia, we concluded that she had hypoglycemic encephalopathy from a self-administered insulin injection. On the 5th day after admission, brain MRI revealed diffuse brain swelling, and DWI clearly showed heterogeneous high-intensity signal areas in the both cortex and subcortex but sparing the motor, sensory and visual centers (Fig. 1 and Fig. 2). On the 7th day, she occasionally opened her eyes but did not respond to verbal commands. On the 11th day, after extubation, she made incomprehensible verbal sounds, spontaneously opened her eyes and moved her extremities with pyramidal tract signs, but did not respond to commands. On the 50th day, almost all the high-intensity signal in the both the cortex and basal ganglia resolved. In addition, marked cerebral atrophy was seen on DWI (Fig. 3). She was totally dependent for self-care and thus was transferred to another hospital after an abortion. Three months later, she remained totally dependent due to aphasia, agnosia and apraxia, but had a normal gait without pyramidal tract signs or ataxia. She remains unchanged 10 months after presentation. Diffusion-weighted MRI predicts prognosis in severe hypoglycemic encephalopathy Yanagawa Y et al. Journal of Clinical Neuroscience 13 (2006) 696–699
. Her blood pressure was 151/110 mmHg; pulse 168 beats per min; tympanic temperature 35.9 °C; and respiratory rate 24 breaths per min. She had isocoric, reactive pupils and ocular bobbing. The remainder of her examination was normal. Arterial blood gas on 6 liters of oxygen by mask revealed pH 7.39, PCO2 38 mmHg, PO2 442 mmHg, base excess −4.0 mmol/L. Her blood glucose was 17 mg/dL and she was immediately infused with 40 ml of 50% glucose to reach 120 mg/dL. A complete blood count showed white blood cells 3200/mm3, red blood cells 423 × 104/mm3 and platelets 41.9 × 104/mm3. Serum biochemistry revealed total bilirubin 0.6 mg/dL, aspartate aminotransferase 26 international units (IU)/L, alanine aminotransferase 12 IU/L, blood urea nitrogen 6 mg/dL, creatinine 0.3 mg/dL, creatine phosphokinase 102 IU/L, sodium 140 mEq/L, potassium 5.0 mEq/L, chloride 99 mEq/L, ammonia 23 mg/dL. A urinary pregnancy test was positive. Cerebrospinal fluid (CSF) analysis showed crystal clear CSF, initial pressure 20 cmH2O and normal cell count, lactate and pyruvate. A computed tomographic scan of her head demonstrated diffuse brain swelling. An electroencephalogram showed low voltage fast waves and no typical epileptic discharges. Abdominal sonography demonstrated a 10-week-old embryo. She was intubated and ventilated in the intensive care unit and brain swelling and raised intracranial pressure was managed with diuresis. Blood glucose was repeatedly low for the first 12 hours, so she received a continuous glucose infusion. After the second hospital day, she was no longer hypoglycemic. On the third hospital day, serum biochemistry revealed insulin 12.5 μU/mL (<17), c-peptide 0.56 ng/mL (0.94–2.80), free T pg/mL (2.47–4.34), free T ng/mL (0.97–1.79), cortisol 20.2 μg/dL. As she had a past history of suicide attempt, clinical features of temporary hypoglycemia, normal endocrine function including insulin, normal lactate and pyruvate in the CSF, and no hypotension or hypoxia, we concluded that she had hypoglycemic encephalopathy from a self-administered insulin injection. On the 5th day after admission, brain MRI revealed diffuse brain swelling, and DWI clearly showed heterogeneous high-intensity signal areas in the both cortex and subcortex but sparing the motor, sensory and visual centers (Fig. 1 and Fig. 2). On the 7th day, she occasionally opened her eyes but did not respond to verbal commands. On the 11th day, after extubation, she made incomprehensible verbal sounds, spontaneously opened her eyes and moved her extremities with pyramidal tract signs, but did not respond to commands. On the 50th day, almost all the high-intensity signal in the both the cortex and basal ganglia resolved. In addition, marked cerebral atrophy was seen on DWI (Fig. 3). She was totally dependent for self-care and thus was transferred to another hospital after an abortion. Three months later, she remained totally dependent due to aphasia, agnosia and apraxia, but had a normal gait without pyramidal tract signs or ataxia. She remains unchanged 10 months after presentation. Diffusion-weighted MRI predicts prognosis in severe hypoglycemic encephalopathy Yanagawa Y et al. Journal of Clinical Neuroscience 13 (2006) 696–699.")
56
Fig 1. Case 1, a 65-year-old man in a diabetic coma with seizures.
glibenclamide and metformin blood glucose was 2.1 mmol/L, no clinical improvement in his level of consciousness, died on the fifteenth

57
69-year-old diabetic man with atrial fibrillation who suddenly became unresponsive, 12 hours later shows complete normalization of previously noted lesions OAD, 1.9 mmol/L, the patient regained consciousness, recovering rapidly and completely after intravenous dextrose Lo L. Diffusion-Weighted MR Imaging in Early Diagnosis and Prognosis of Hypoglycemia Am J Neuroradiol 27:1222–24 Jun-Jul 2006

58
KEZELÉSI MÓD és SZÖVŐDMÉNYEK
Gépkocsi vezetés Fegyveres testületek, tüzoltók MACOSZ Dr. Fövényi József KEZELÉSI MÓD és SZÖVŐDMÉNYEK Diéta, orális Magán gépkocsi- más kizáró ok hiányában alkalmas Ismert cukorbetegség- hivatásos jogosítványra nem alkalmas Korábbi hivatásos jogosítvány- bizonyos járműveket vezethet Inzulinnal egyensúlyban Magán gépkocsi- diabetológus szakorvos véleménye alapján alkalmas lehet Hivatásos jogosítványt nem szerezhet Korábbi hivatásos- diabetológus vélemény alapján alkalmas, Kivéve csoportos személyszállító járműveket

59
Inzulin elválasztást fokozó szerek- hipoglikéma miatt
Foglalkozási kockázat: pilóta, tömegközlekedés, öntöde, bányászat Inzulinnal kezelt- hivatásos gépjárművezető (vonat, busz, troli, villamos, metro) Kamion sofőr Légiközlekedés (polgári, katona, repülő, helikopter) fegyveres testületek, katasztrófa elhárítás, honvédelem, rendőrség, biztonsági szolgálat, fegyőr, tűzoltó) Vadászati engedély: egyéni elbírálás Veszélyes munkakörök: bányászat, öntöde, magasban, magasfeszültség)
 Kamion sofőr. Légiközlekedés. (polgári, katona, repülő, helikopter) fegyveres testületek, katasztrófa elhárítás, honvédelem, rendőrség, biztonsági szolgálat, fegyőr, tűzoltó) Vadászati engedély: egyéni elbírálás. Veszélyes munkakörök: bányászat, öntöde, magasban, magasfeszültség)")
60
Magyar Közlöny 2009. 153-ik száma 57/209 (10. 30
Magyar Közlöny ik száma 57/209 ( ) ILM-ÖM-PTNM Igazságügyi és Rendészeti, Önkormányzati és a Polgári Nemzetbiztonsági Szolgálatokat irányító Miniszterek által kiadott közös rendeletben szabályozták a fegyveres testület tagjainak alkalmassági vizsgálatát
 ILM-ÖM-PTNM Igazságügyi és Rendészeti, Önkormányzati és a Polgári Nemzetbiztonsági Szolgálatokat irányító Miniszterek által kiadott közös rendeletben szabályozták a fegyveres testület tagjainak alkalmassági vizsgálatát.")
61
016 Diab- mell. I II III IV S K BNO 1 Diétával kezelhető Jó általános állapot E E10-14 2 Szigorú diétával, tablettával kezelhető AN AS E 10-14

62
3 Szigorú diétával, közepes mennyiségű insulinnal kezelhető, nem labilis jó általános állapot AN E E10-14 4 Szigorú diétával nagy mennyiségű insulinnal kezelhető, labilis formák, érszövődmények

63
1DM 6 hónapos megelőző időszak jó anyagcsere vezetése
2DM insulin kezelése esetén 3 hónap megelőző időszak jó anyagcsere vezetése vércukorellenőrzés diétával 1 vagy 2 alkalom hetente metformin thiazolidindion és alfa glucosidase 1 vagy 2x hetente, sulfanylurea, meglitinid, nateglinid 2x naponta, reggel és vacsorakor, illetve bármilyen hypoglycaemiára gyanús eseménykor, 1x adott insulin esetén oralis kezeléssel való kombinációban 2x naponta, 2 vagy többszöri insulin alkalmazás vagy pumpa naponta 3-4x, étkezésekkor és lefekvéskor illetve a hypoglycaemiára gyanus események idején. Előírják három havonta, évi 4x a HbA1c ellenőrzést 8%-nál magasabb, akkor a beállítás módosítását. Az alkalmassági vizsgálatot megelőző évben ne legyen a munkavégzést lehetetlenné tevő hypoglycaemiás epizód és az előző három évben ne forduljon elő kettőnél többször, illetve a diagnózis felállításától számítva ne legyen kettőnél többször súlyos hypoglycaemias epizód (eszméletvesztés vagy külső segítséget igénylő glucagon, vagy glukóz beavatkozás) Ne legyen nem észlelt/tudatosult hypoglycaemias periódus (vércukor 60 mg/dl= 3.33 mmol/l alatt) ACOEM a Guidance for the Medical Evaluation of Law Enforcement Offices IV/3 diabetesre vonatkozó fejezete [F1] [F2]
 Ne legyen nem észlelt/tudatosult hypoglycaemias periódus (vércukor 60 mg/dl= 3.33 mmol/l alatt) ACOEM a Guidance for the Medical Evaluation of Law Enforcement Offices IV/3 diabetesre vonatkozó fejezete. [F1] [F2]")
64
21. FEJEZET. ENDROKRINOLÓGIAI KÁROSODÁSOK
LEÖVEY ANDRÁS, HALMOS TAMÁS, JUHÁSZ FERENC

65
Sebészileg kezelt hypogycaemia
A károsodás kritériuma ÖEK %-a I. osztály Sebészileg gyógyított hypoglykaemia –5 II. osztály Kimutatott hypoglykaemia a tünetek súlyosságától függôen, pl. 50% insulinoma –50 Köszönöm a figyelmet

Hasonló előadás